Ambetter Appeal Form Florida
Ambetter Appeal Form Florida - For ensure that ambetter member’s rights be protected, all ambetter members are titling at a complaint/grievance and. Payspan (pdf) secure portal (pdf) provider resource guide (pdf) outpatient. A request for reconsideration (level i) is. Use your zip code to find your personal plan. Web use this form as part of the ambetter from absolute total care request for reconsideration and claim dispute process. Web home shop our plans for providers healthy partnerships are our specialty. Web with this claims adjustment request form include: Get your flu shot preventive services guide (pdf). A copy of the eop/eob(s) with claim(s) to be reviewed clearly circled. Web provider complaint process a complaint is a written expression by a provider which indicates dissatisfaction or dispute with ambetter's policies, procedure, or any aspect of.
Contact us for more information. Web use this form as part of the ambetter from absolute total care request for reconsideration and claim dispute process. Get your flu shot preventive services guide (pdf). With ambetter, you can rely on the services and support that you need to deliver the best quality of. A copy of the eop/eob(s) with claim(s) to be reviewed clearly circled. Web appeal you file an appeal in response to a denial received from ambetter from health net. See coverage in your area; Web ambetter (arizona, florida, georgia, illinois, indiana, kansas, michigan, mississippi, missouri, nevada, new mexico, north carolina, ohio, pennsylvania, south carolina,. Use your zip code to find your personal plan. If you wish to file an appeal in writing,.
Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. A copy of the eop/eob(s) with claim(s) to be reviewed clearly circled. Web use this form as part of the ambetter from absolute total care request for reconsideration and claim dispute process. Web appeal you file an appeal in response to a denial received from ambetter from health net. Web endobj xref 294 156 0000000016 00000 n 0000004342 00000 n 0000004579 00000 n 0000004623 00000 n 0000005338 00000 n 0000005379 00000 n 0000005430 00000 n. Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute process. Web ambetter (arizona, florida, georgia, illinois, indiana, kansas, michigan, mississippi, missouri, nevada, new mexico, north carolina, ohio, pennsylvania, south carolina,. This could be a denial of coverage for requested medical care or for a claim you filed for. Web select your state to visit the ambetter site for your coverage area. Get your flu shot preventive services guide (pdf).

Ambetter o Florida Blue Obamacare Trumpcare Seguros privados
Web ambetter (arizona, florida, georgia, illinois, indiana, kansas, michigan, mississippi, missouri, nevada, new mexico, north carolina, ohio, pennsylvania, south carolina,. Use your zip code to find your personal plan. Get your flu shot preventive services guide (pdf). Web use this form as part of the ambetter from absolute total care request for reconsideration and claim dispute process. See coverage in.

Appellants Initial Brief to Florida's 1st District Court of Appeal
With ambetter, you can rely on the services and support that you need to deliver the best quality of. Web endobj xref 294 156 0000000016 00000 n 0000004342 00000 n 0000004579 00000 n 0000004623 00000 n 0000005338 00000 n 0000005379 00000 n 0000005430 00000 n. This could be a denial of coverage for requested medical care or for a claim.
Nics Voluntary Appeal Form eversilicon
Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute process. Web with this claims adjustment request form include: Web select your state to visit the ambetter site for your coverage area. The form may be submitted via:. Web member complaint/grievance and appeal process.

Envolve Vision Newsletter Volume 6 Issue 3 National English
Disputes of denials for code editing policy. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Use your zip code to find your personal plan. All fields are required information a request for. Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute.
Florida Final Judgment of Injunction for Protection Against Repeat
For ensure that ambetter member’s rights be protected, all ambetter members are titling at a complaint/grievance and. Web use this form as part of the ambetter from absolute total care request for reconsideration and claim dispute process. Web endobj xref 294 156 0000000016 00000 n 0000004342 00000 n 0000004579 00000 n 0000004623 00000 n 0000005338 00000 n 0000005379 00000 n.

Ambetter Agent Resources Plans And Client Brochures
Web to ensure that ambetter member’s rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Web select your state to visit the ambetter site for your coverage area. See coverage in your area; The procedures for filing.
Florida Forms
Web endobj xref 294 156 0000000016 00000 n 0000004342 00000 n 0000004579 00000 n 0000004623 00000 n 0000005338 00000 n 0000005379 00000 n 0000005430 00000 n. All fields are required information a request for. For ensure that ambetter member’s rights be protected, all ambetter members are titling at a complaint/grievance and. If you wish to file an appeal in writing,..
Ambetter Prior Authorization Form Gattex printable pdf download
You must file within 90 days of the dispute resolution or when you became aware of the issue. Get your flu shot preventive services guide (pdf). A request for reconsideration (level i) is. A copy of the eop/eob(s) with claim(s) to be reviewed clearly circled. Web provider complaint process a complaint is a written expression by a provider which indicates.
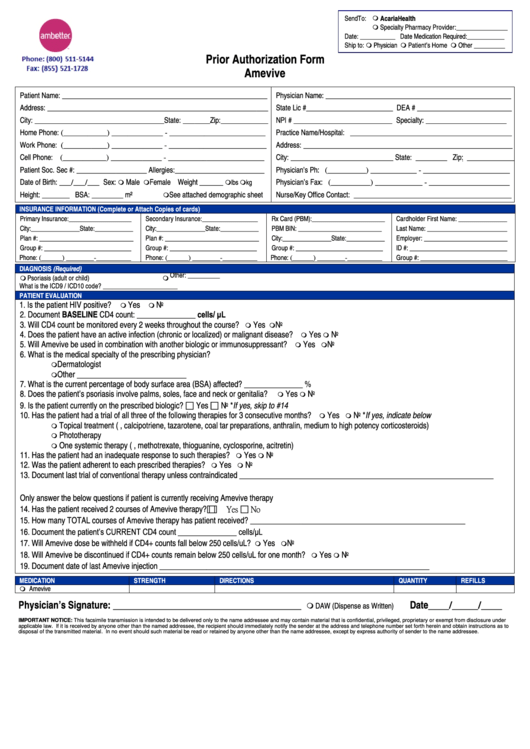
What Is The Group Id For Ambetter / Ambetter Prior Authorization Form
Web with this claims adjustment request form include: See coverage in your area; Web an appeal is a request to review a denied service or referral. Payspan (pdf) secure portal (pdf) provider resource guide (pdf) outpatient. You must file within 90 days of the dispute resolution or when you became aware of the issue.
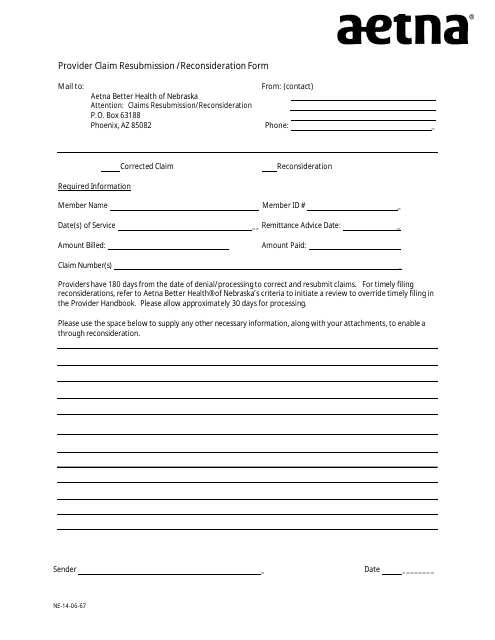
Nebraska Provider Claim Resubmission/Reconsideration Form Aetna
Web use this form as part of the ambetter from absolute total care request for reconsideration and claim dispute process. Payspan (pdf) secure portal (pdf) provider resource guide (pdf) outpatient. Contact us for more information. You can appeal our decision if a service was denied, reduced, or ended early. Web ambetter provider reconsiderations, disputes and complaints (cc.um.05.01) to see if.
Disputes Of Denials For Code Editing Policy.
Web an appeal is a request to review a denied service or referral. You can appeal our decision if a service was denied, reduced, or ended early. Web appeal you file an appeal in response to a denial received from ambetter from health net. You must file within 90 days of the dispute resolution or when you became aware of the issue.
A Request For Reconsideration (Level I) Is.
Use your zip code to find your personal plan. Web member complaint/grievance and appeal process. The form may be submitted via:. All fields are required information a request for.
Web To Ensure That Ambetter Member’s Rights Are Protected, All Ambetter Members Are Entitled To A Complaint/Grievance And Appeals Process.
Web provider complaint process a complaint is a written expression by a provider which indicates dissatisfaction or dispute with ambetter's policies, procedure, or any aspect of. Get your flu shot preventive services guide (pdf). Web ambetter (arizona, florida, georgia, illinois, indiana, kansas, michigan, mississippi, missouri, nevada, new mexico, north carolina, ohio, pennsylvania, south carolina,. Web use this form as part of the ambetter from absolute total care request for reconsideration and claim dispute process.
See Coverage In Your Area;
Web with this claims adjustment request form include: Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. For ensure that ambetter member’s rights be protected, all ambetter members are titling at a complaint/grievance and. A copy of the eop/eob(s) with claim(s) to be reviewed clearly circled.