Cms 1500 Form Sample
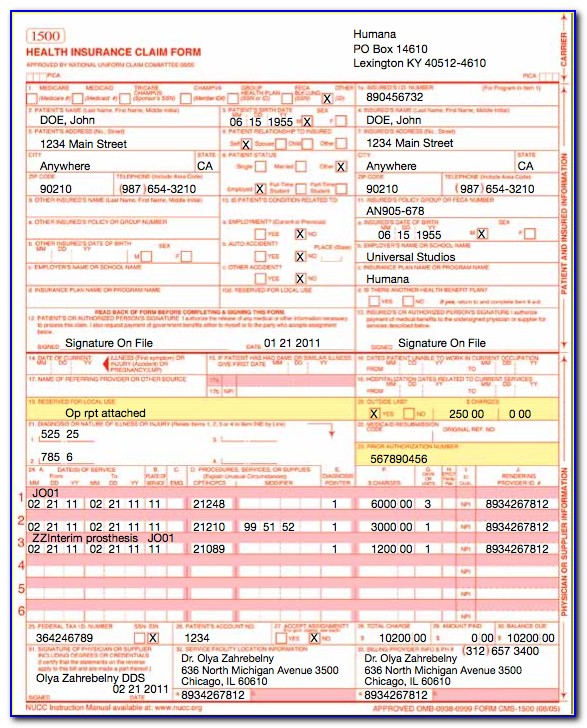
Cms 1500 Form Sample - Last updated wed, 04 jan 2023 13:36:02 +0000. It can be purchased in any version required by calling the u.s. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. You'll see instructions on how to complete the field. Number (for program in item 1) 4. You may also click in any field for more detailed instructions. Insured’s policy group or feca number a. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Insured’s address (no., street) city state zip code telephone (include area code) 11. Insured’s name (last name, first name, middle initial) 7.
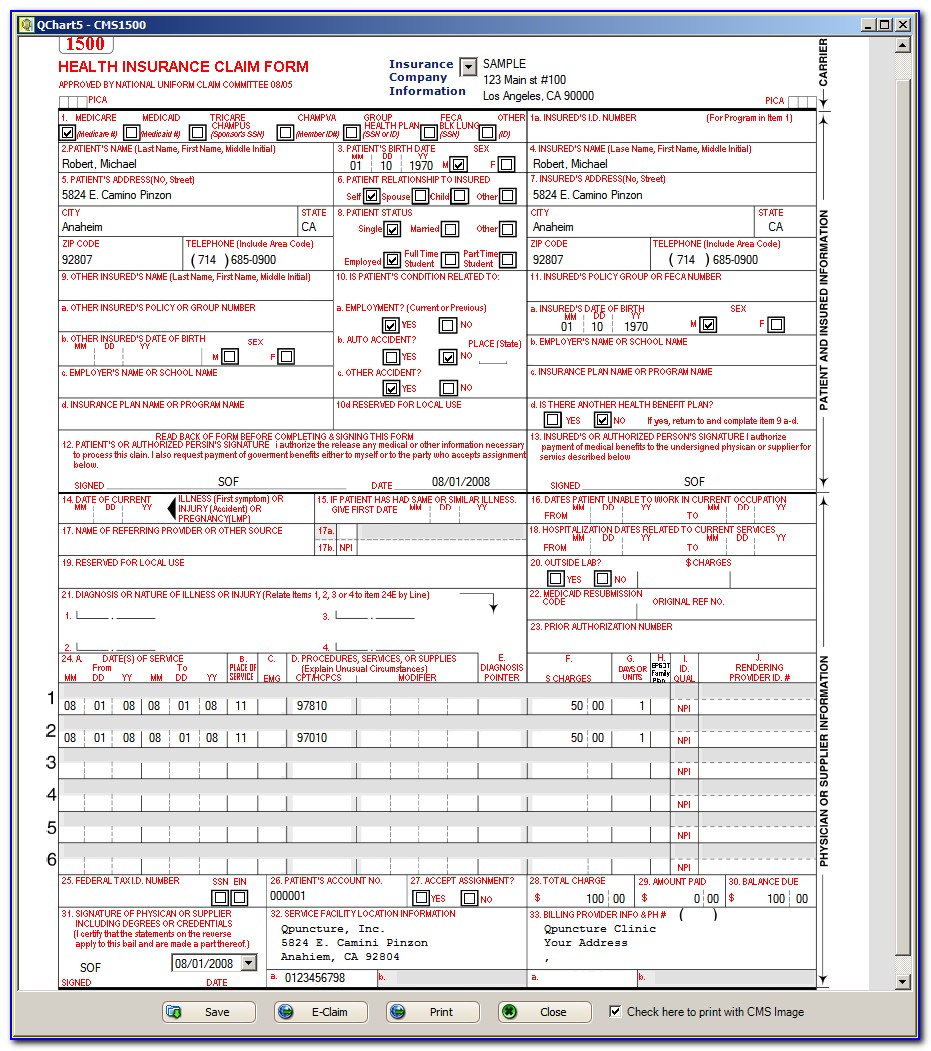
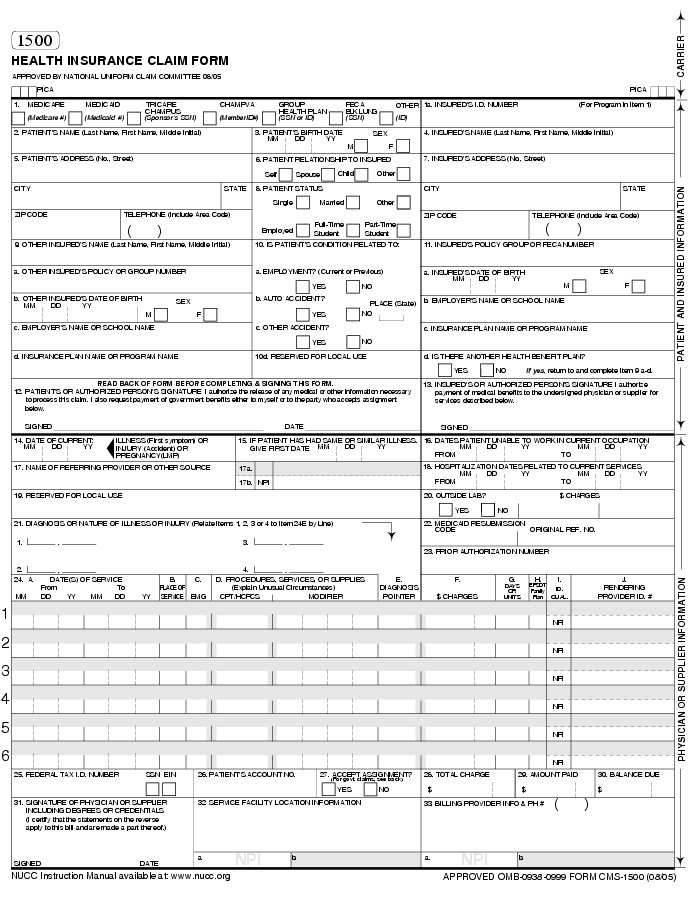
The patient was seen for an office visit. Insured’s name (last name, first name, middle initial) 7. You'll see instructions on how to complete the field. Number (for program in item 1) 4. Insured’s policy group or feca number a. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. You may also click in any field for more detailed instructions. It can be purchased in any version required by calling the u.s. Last updated wed, 04 jan 2023 13:36:02 +0000.
The patient was seen for an office visit. You may also click in any field for more detailed instructions. Insured’s name (last name, first name, middle initial) 7. You'll see instructions on how to complete the field. Last updated wed, 04 jan 2023 13:36:02 +0000. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Insured’s address (no., street) city state zip code telephone (include area code) 11. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. It can be purchased in any version required by calling the u.s. Insured’s policy group or feca number a.

Sample Cms 1500 Form Completed Form Resume Examples Mj1vgOlKwy
You may also click in any field for more detailed instructions. You'll see instructions on how to complete the field. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office.

Example Of Cms 1500 Form Completed Form Resume Examples nO9bvnp94D
The patient was seen for an office visit. It can be purchased in any version required by calling the u.s. Insured’s policy group or feca number a. You may also click in any field for more detailed instructions. You'll see instructions on how to complete the field.

cms1500claimformsample CASO Document Management
Insured’s address (no., street) city state zip code telephone (include area code) 11. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Insured’s policy group or feca number a. It can be purchased in any version required by calling the u.s. The.
Completed Cms 1500 Claim Form Sample Form Resume Examples K75PBGVkl2
Insured’s policy group or feca number a. Insured’s name (last name, first name, middle initial) 7. Insured’s address (no., street) city state zip code telephone (include area code) 11. It can be purchased in any version required by calling the u.s. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers.
Recording Additional Information on the CMS 1500 Form & ANSI File
It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Insured’s name (last name, first name, middle initial) 7. It can be purchased in any version required by calling the u.s. Insured’s address (no., street) city state zip code telephone (include area code).
Sample new CMS 1500 CLAIM form CMS 1500 claim form and UB 04 form
Insured’s address (no., street) city state zip code telephone (include area code) 11. You may also click in any field for more detailed instructions. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. The 1500 health insurance claim form (1500 claim form).

Cms 1500 Form 0212 Software Universal Network
Insured’s address (no., street) city state zip code telephone (include area code) 11. It can be purchased in any version required by calling the u.s. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Number (for program in item 1) 4. You.
![Mental Health CMS1500 Form [Download JPG + PDF]](https://therathink.com/wp-content/uploads/2017/03/CMS-1500-New-Format.jpg)
Mental Health CMS1500 Form [Download JPG + PDF]
Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. The patient was seen for an office visit. Insured’s policy group or feca number a. Insured’s name (last name, first name,.
Sample 1500 Claim Form Filled Out Form Resume Examples a15qXrADeQ
Number (for program in item 1) 4. You may also click in any field for more detailed instructions. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Insured’s policy group or feca number a. It can be purchased in any version required.
cms claimbilling CMS 1500 claim form billing instruction Part 1
Insured’s name (last name, first name, middle initial) 7. Insured’s policy group or feca number a. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. You'll see instructions on how to complete the field. You may also click in any field for more detailed instructions.
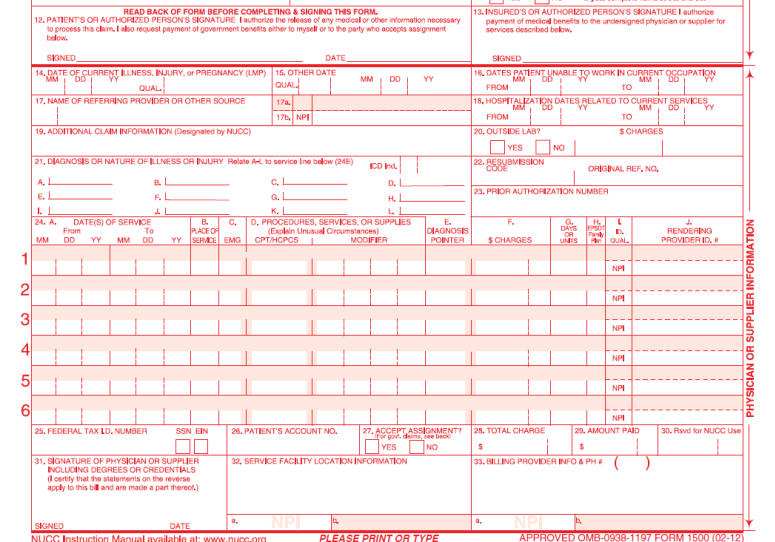
Insured’s Name (Last Name, First Name, Middle Initial) 7.
The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Insured’s address (no., street) city state zip code telephone (include area code) 11. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim.
Last Updated Wed, 04 Jan 2023 13:36:02 +0000.
Insured’s policy group or feca number a. It can be purchased in any version required by calling the u.s. The patient was seen for an office visit. You'll see instructions on how to complete the field.
You May Also Click In Any Field For More Detailed Instructions.
Number (for program in item 1) 4.