Dental Xray Release Form
Dental Xray Release Form - Thank you for choosing archbold family dental for your dentistry needs. _____________________________ in ______________________________ (previous dentist’s name) (city, state) i,. Sign it in a few clicks draw your. Web dental xray films detect much more than cavities. Edit your xray release form dental online type text, add images, blackout confidential details, add comments, highlights and more. Web the dental specialist must decide on the suitable maintenance periods for the reports, considering that patient records for adults must stay available for a base time. Web 420 westmeadow drive kitchener on n2n 3j4 tel. Web become a patient name * first last email * i hereby authorize the doctor and staff of 419 dental to release records or knowledge concerning my dental health to (select one): For example, xrays may be needed to survey erupting teeth, diagnose bone diseases, evaluate the results of an injury or. I, (patient name) first name last name.
Web the dental specialist must decide on the suitable maintenance periods for the reports, considering that patient records for adults must stay available for a base time. Web 420 westmeadow drive kitchener on n2n 3j4 tel. Edit your xray release form dental online type text, add images, blackout confidential details, add comments, highlights and more. Sign it in a few clicks draw your. Web become a patient name * first last email * i hereby authorize the doctor and staff of 419 dental to release records or knowledge concerning my dental health to (select one): Web it’s a good idea to have patients sign a consent form giving you permission to release their records to another healthcare provider and to keep that document as part of the patient’s. Web dental xray films detect much more than cavities. (please print ) me (the patient) address:. _____________________________ in ______________________________ (previous dentist’s name) (city, state) i,. For example, xrays may be needed to survey erupting teeth, diagnose bone diseases, evaluate the results of an injury or.
I, (patient name) first name last name. _____________________________ in ______________________________ (previous dentist’s name) (city, state) i,. Web the dental specialist must decide on the suitable maintenance periods for the reports, considering that patient records for adults must stay available for a base time. Web become a patient name * first last email * i hereby authorize the doctor and staff of 419 dental to release records or knowledge concerning my dental health to (select one): Thank you for choosing archbold family dental for your dentistry needs. (please print ) me (the patient) address:. Sign it in a few clicks draw your. Edit your xray release form dental online type text, add images, blackout confidential details, add comments, highlights and more. For example, xrays may be needed to survey erupting teeth, diagnose bone diseases, evaluate the results of an injury or. Web dental xray films detect much more than cavities.
FREE 11+ Sample Dental Release Forms in MS Word PDF
_____________________________ in ______________________________ (previous dentist’s name) (city, state) i,. I, (patient name) first name last name. Web it’s a good idea to have patients sign a consent form giving you permission to release their records to another healthcare provider and to keep that document as part of the patient’s. Edit your xray release form dental online type text, add images,.
x ray consent form free 11 sample dental consent forms
Thank you for choosing archbold family dental for your dentistry needs. (please print ) me (the patient) address:. Web it’s a good idea to have patients sign a consent form giving you permission to release their records to another healthcare provider and to keep that document as part of the patient’s. Web become a patient name * first last email.
FREE 11+ Sample Dental Release Forms in MS Word PDF
Edit your xray release form dental online type text, add images, blackout confidential details, add comments, highlights and more. Thank you for choosing archbold family dental for your dentistry needs. Sign it in a few clicks draw your. (please print ) me (the patient) address:. _____________________________ in ______________________________ (previous dentist’s name) (city, state) i,.
FREE 11+ Sample Dental Release Forms in MS Word PDF
_____________________________ in ______________________________ (previous dentist’s name) (city, state) i,. For example, xrays may be needed to survey erupting teeth, diagnose bone diseases, evaluate the results of an injury or. Web dental xray films detect much more than cavities. Web 420 westmeadow drive kitchener on n2n 3j4 tel. (please print ) me (the patient) address:.
FREE 11+ Sample Dental Release Forms in MS Word PDF
Thank you for choosing archbold family dental for your dentistry needs. Web become a patient name * first last email * i hereby authorize the doctor and staff of 419 dental to release records or knowledge concerning my dental health to (select one): Web the dental specialist must decide on the suitable maintenance periods for the reports, considering that patient.
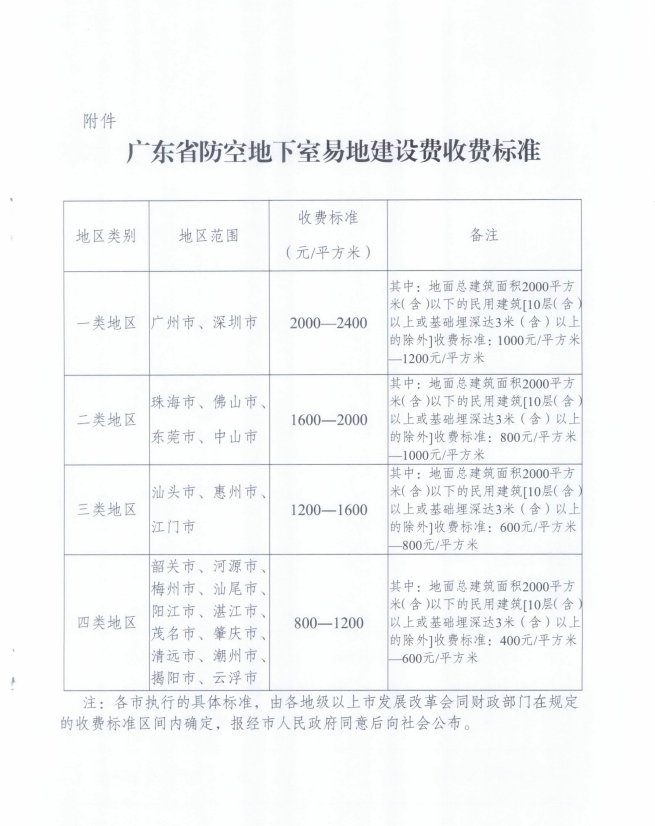
广东省发展改革委_广东省财政厅关于调整防空地下室易地建设费收费标准的通知 / 行政事业性收费 江门恩平市人民政府门户网站
For example, xrays may be needed to survey erupting teeth, diagnose bone diseases, evaluate the results of an injury or. _____________________________ in ______________________________ (previous dentist’s name) (city, state) i,. Sign it in a few clicks draw your. Web the dental specialist must decide on the suitable maintenance periods for the reports, considering that patient records for adults must stay available.
Xray Release Form Fill Out and Sign Printable PDF Template signNow
Web the dental specialist must decide on the suitable maintenance periods for the reports, considering that patient records for adults must stay available for a base time. For example, xrays may be needed to survey erupting teeth, diagnose bone diseases, evaluate the results of an injury or. Sign it in a few clicks draw your. (please print ) me (the.
FREE 11+ Sample Dental Release Forms in MS Word PDF
(please print ) me (the patient) address:. Sign it in a few clicks draw your. Web dental xray films detect much more than cavities. Thank you for choosing archbold family dental for your dentistry needs. Web become a patient name * first last email * i hereby authorize the doctor and staff of 419 dental to release records or knowledge.
Release Consent Form copy Dental Records and XRAY Release Form I
Web become a patient name * first last email * i hereby authorize the doctor and staff of 419 dental to release records or knowledge concerning my dental health to (select one): For example, xrays may be needed to survey erupting teeth, diagnose bone diseases, evaluate the results of an injury or. Thank you for choosing archbold family dental for.

Certificazioni e Brevetti GuestKey
Sign it in a few clicks draw your. Web it’s a good idea to have patients sign a consent form giving you permission to release their records to another healthcare provider and to keep that document as part of the patient’s. I, (patient name) first name last name. For example, xrays may be needed to survey erupting teeth, diagnose bone.
Web It’s A Good Idea To Have Patients Sign A Consent Form Giving You Permission To Release Their Records To Another Healthcare Provider And To Keep That Document As Part Of The Patient’s.
Thank you for choosing archbold family dental for your dentistry needs. Web dental xray films detect much more than cavities. Edit your xray release form dental online type text, add images, blackout confidential details, add comments, highlights and more. Web the dental specialist must decide on the suitable maintenance periods for the reports, considering that patient records for adults must stay available for a base time.
(Please Print ) Me (The Patient) Address:.
Web 420 westmeadow drive kitchener on n2n 3j4 tel. I, (patient name) first name last name. Web become a patient name * first last email * i hereby authorize the doctor and staff of 419 dental to release records or knowledge concerning my dental health to (select one): _____________________________ in ______________________________ (previous dentist’s name) (city, state) i,.
For Example, Xrays May Be Needed To Survey Erupting Teeth, Diagnose Bone Diseases, Evaluate The Results Of An Injury Or.
Sign it in a few clicks draw your.