Designation Of Personal Representative Form
Designation Of Personal Representative Form - The individual named as my personal representative may act on my behalf in regard to my healthcare coverage through blue cross & blue shield of. Register and subscribe now to work on your allways personal representative designation req Web university of pittsburgh medical center (upmc) personal representative designation form dear patient: We understand that you wish to appoint a personal representative to act on your behalf as described below. Web designation of personal representative you may designate a personal representative who will act on your behalf in making decisions related to health care, which includes. Print, sign and bring your completed form to your provider. Designation of personal representative patient identification name mr#. University of pittsburgh medical center (upmc) personal. Web by completing this form you are informing us of your wish to designate the named person as your personal representative. I no longer wish to have a representative.
The individual named as my personal representative may act on my behalf in regard to my healthcare coverage through blue cross & blue shield of. University of pittsburgh medical center (upmc) personal. We understand that you wish to appoint a personal representative to act on your behalf as described below. I no longer wish to have a representative. Web representative’s mailing address (street, po box, city, state, zip code) representative’s telephone number to represent the above named property owner before the state. Web designation of personal representative. If you have a case before us and need assistance, you can appoint a representative to help you. Print, sign and bring your completed form to your provider. Web up to 8% cash back to designate or remove your personal representative, please download the necessary forms below. Web university of pittsburgh medical center (upmc) personal representative designation form dear patient:
See page 2 for return instructions. Designation of personal representative patient identification name mr#. I no longer wish to have a representative. Web personal representative designation form dear patient: To allow a family member, other relative, or a close personal friend to have access to protected information. Print, sign and bring your completed form to your provider. Web my total and permanent disability request. The individual named as my personal representative may act on my behalf in regard to my healthcare coverage through blue cross & blue shield of. Web by completing this form you are informing us of your wish to designate the named person. By signing this form you indicate that you have voluntarily chosen the attorney designated below to serve as your.
Form HFS3806F Download Fillable PDF or Fill Online Personal
If you have a case before us and need assistance, you can appoint a representative to help you. Web two identifiers needed hereby designate the following personal representative to assist my child in exercising my health information rights under the new hampshire patients’. University of pittsburgh medical center (upmc) personal. We understand that you wish to appoint a personal representative.
Hawaii Designation of Representative and Certificate of Service
Web designation of personal legal representative osc case no. By signing this form you indicate that you have voluntarily chosen the attorney designated below to serve as your. Web personal representative designation form dear patient: Web personal representative may either be legally appointed, or designated by a customer to act on his or her behalf: Web designation of personal representative.

Uhc Designation Of Authorized Representative Form
Designation of personal representative form (pdf) spanish version (pdf) designation of personal. Please provide contact information for the representative that you are. Web university of pittsburgh medical center (upmc) personal representative designation form dear patient: If you have a case before us and need assistance, you can appoint a representative to help you. When a personal representative has been legally.
Fillable Form Dss1688 Designation Of Authorized Representative
To allow a family member, other relative, or a close personal friend to have access to protected information. Web designation of personal legal representative osc case no. I no longer wish to have a representative. Web designation of personal representative. By signing this form you indicate that you have voluntarily chosen the attorney designated below to serve as your.
Oath of Personal Representative & Designation & Acceptance of Resident
Web representative’s mailing address (street, po box, city, state, zip code) representative’s telephone number to represent the above named property owner before the state. Web designation of personal legal representative osc case no. By signing this form you indicate that you have voluntarily chosen the attorney designated below to serve as your. University of pittsburgh medical center (upmc) personal. Web.
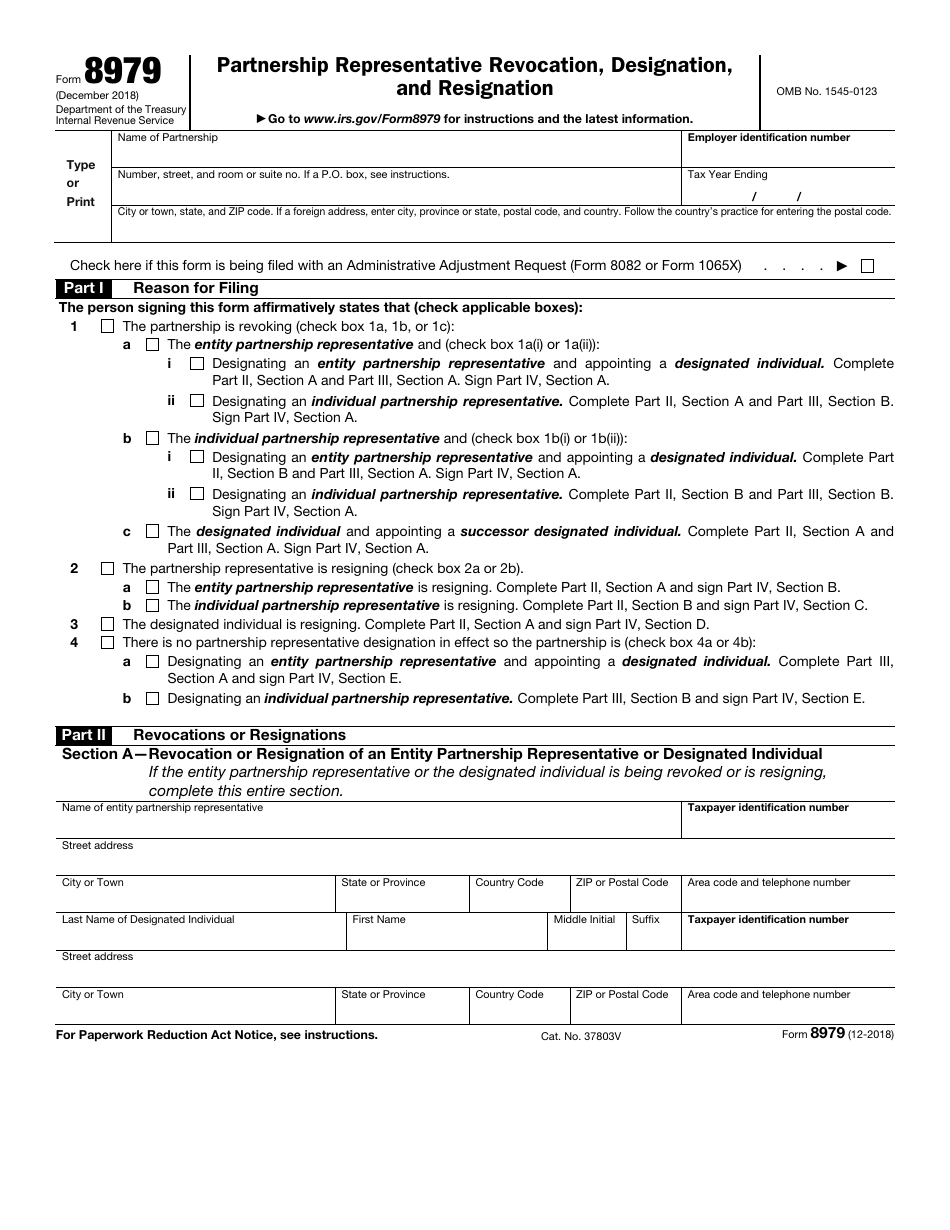
IRS Form 8979 Download Fillable PDF or Fill Online Partnership
Designation of personal representative patient identification name mr#. See page 2 for return instructions. Web best interest to treat the person as your personal representative. Web designation of personal representative you may designate a personal representative who will act on your behalf in making decisions related to health care, which includes. Web i hereby designate the following personal representative to.

Member Designation of Representative to Inspect and Copy Documents
Web two identifiers needed hereby designate the following personal representative to assist my child in exercising my health information rights under the new hampshire patients’. Web by completing this form you are informing us of your wish to designate the named person. Web please fill out one of the following forms and mail or return it to us: If you.
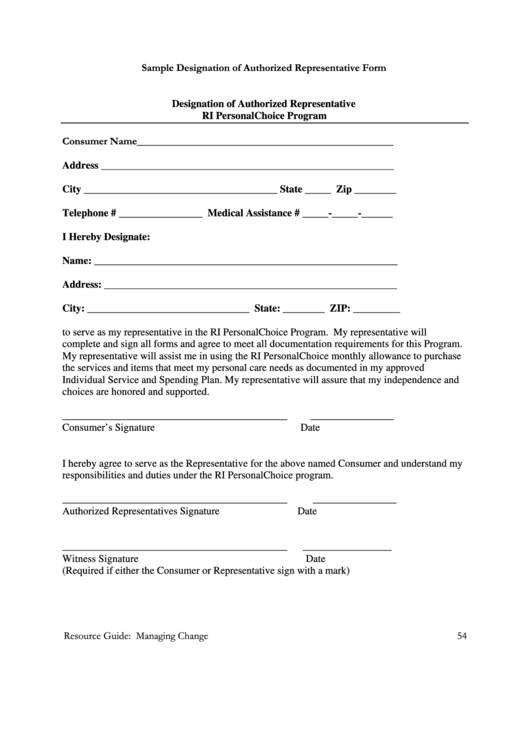
Sample Designation Of Authorized Representative Form printable pdf download
Web up to 8% cash back to designate or remove your personal representative, please download the necessary forms below. When a personal representative has been legally appointed,. To allow a family member, other relative, or a close personal friend to have access to protected information. University of pittsburgh medical center (upmc) personal. A personal representative designation will remain in effect.
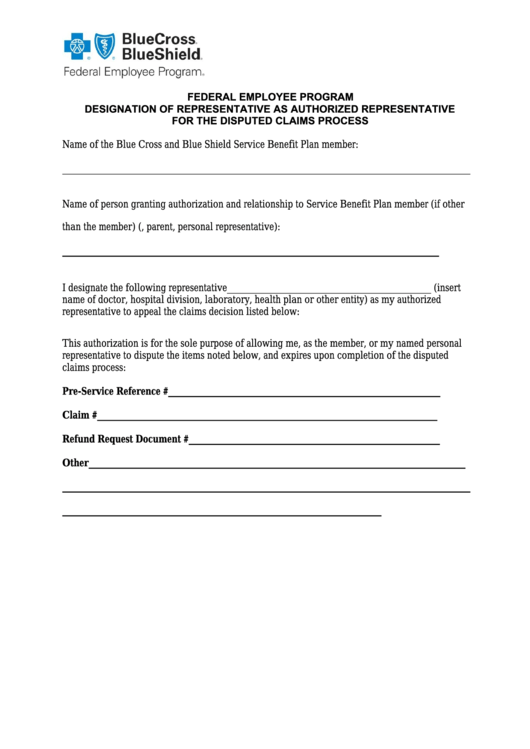
Designation Of Representative As Authorized Representative For The
If you have a case before us and need assistance, you can appoint a representative to help you. Web two identifiers needed hereby designate the following personal representative to assist my child in exercising my health information rights under the new hampshire patients’. Web personal representative may either be legally appointed, or designated by a customer to act on his.
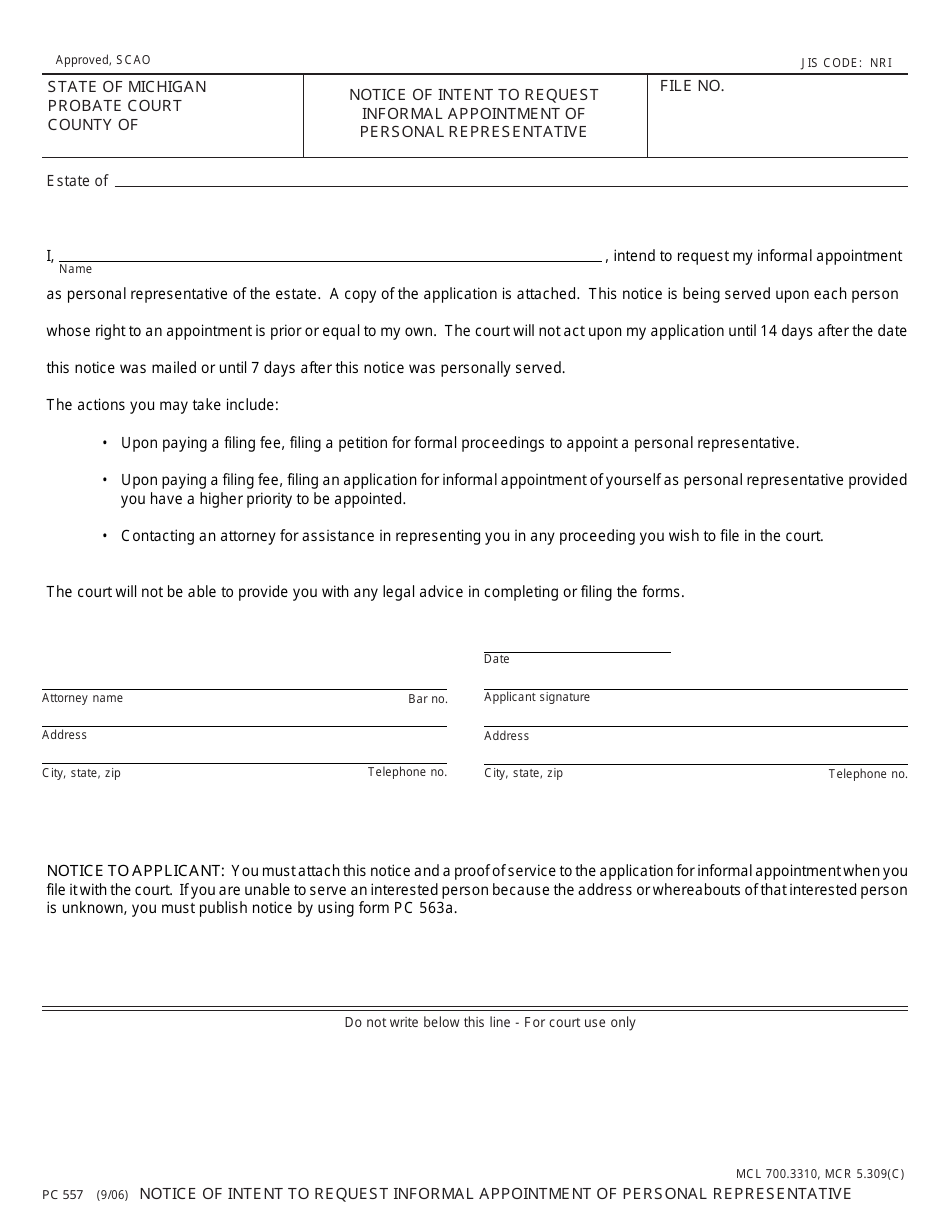
Form PC557 Download Fillable PDF or Fill Online Notice of Intent to
Designation of personal representative form (pdf) spanish version (pdf) designation of personal. Print, sign and bring your completed form to your provider. Web university of pittsburgh medical center (upmc) personal representative designation form dear patient: Web designation of personal representative you may designate a personal representative who will act on your behalf in making decisions related to health care, which.
We Understand That You Wish To Appoint A Personal Representative To Act On Your Behalf As Described Below.
To allow a family member, other relative, or a close personal friend to have access to protected information. A personal representative designation will remain in effect until the member, a court order, or an. Web my total and permanent disability request. Web up to 8% cash back to designate or remove your personal representative, please download the necessary forms below.
Web Representative’s Mailing Address (Street, Po Box, City, State, Zip Code) Representative’s Telephone Number To Represent The Above Named Property Owner Before The State.
I no longer wish to have a representative. By signing this form you indicate that you have voluntarily chosen the attorney designated below to serve as your. Web personal representative may either be legally appointed, or designated by a customer to act on his or her behalf: The individual named as my personal representative may act on my behalf in regard to my healthcare coverage through blue cross & blue shield of.
See Page 2 For Return Instructions.
Web by completing this form you are informing us of your wish to designate the named person. Web designation of personal legal representative osc case no. Web best interest to treat the person as your personal representative. Web personal representative designation form dear patient:
Edit, Sign And Save Allways Persnl Designation Req Form.
Web by completing this form you are informing us of your wish to designate the named person as your personal representative. Web i hereby designate the following personal representative to assist me in exercising my health information rights under the new hampshire patients’ bill of rights and the federal. Web designation of personal representative. Web university of pittsburgh medical center (upmc) personal representative designation form dear patient: