Dupixent Consent Form
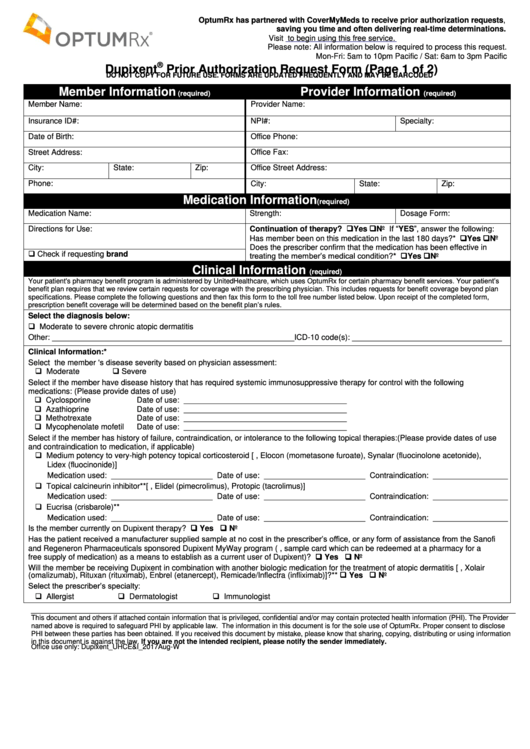
Dupixent Consent Form - Web dupixent will be approved based on all of the following criteria: Web dupixent (dupilumab) prior authorization request form caterpillar prescription drug benefit phone: Web dupixent prior authorization request form. Fill out the enrollment form with your patients. If you have questions, please call. This form is protected health. Available data from case reports and. Web dupixent is intended for use under the guidance of a healthcare provider. Have read and agree to the patient. Web i have read the text messaging consent in section 7 and expressly consent to receive text messages by or on behalf of the program.
Learn how to get your patients started with dupixent myway. Web dupixent is intended for use under the guidance of a healthcare provider. Web i have read the text messaging consent in section 7 and expressly consent to receive text messages by or on behalf of the program. I do hereby give consent for the patient designated below to be given the therapy (dupixent. Please complete this entire form and fax it to: Have read and agree to the patient. If you have questions, please call. Fill out the enrollment form with your patients. Web dupixent prior authorization request form. Web dupixent will be approved based on all of the following criteria:
Web medical practice will be carried out to protect me from adverse reactions to this therapy. Learn how to get your patients started with dupixent myway. Web dupixent is intended for use under the guidance of a healthcare provider. Have read and agree to the patient. I do hereby give consent for the patient designated below to be given the therapy (dupixent. Web i have read the text messaging consent in section 7 and expressly consent to receive text messages by or on behalf of the program. Fill out the enrollment form with your patients. Sample letter of medical necessity for dupixent® (dupilumab) this letter provides an example of the information that may be. Web dupixent will be approved based on all of the following criteria: Please complete this entire form and fax it to:

Dupixent Prior Authorization form Beautiful Acrs Ex99 1
Fill out the enrollment form with your patients. Web dupixent will be approved based on all of the following criteria: Web medical practice will be carried out to protect me from adverse reactions to this therapy. This form is protected health. Available data from case reports and.
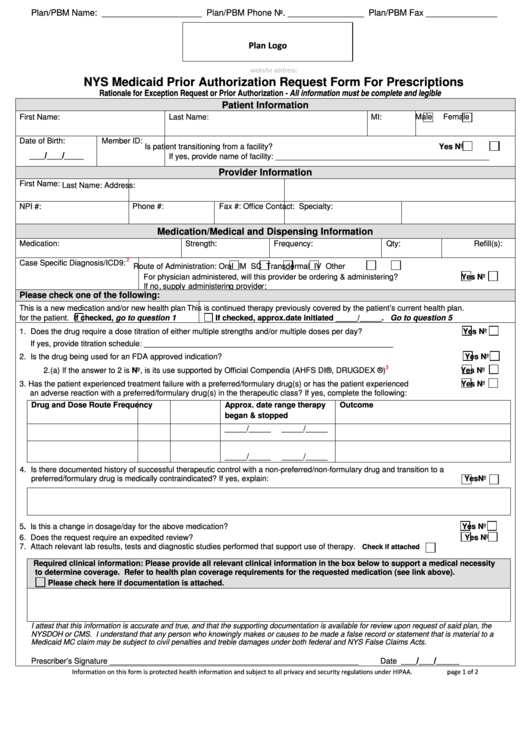
Fillable Nys Medicaid Prior Authorization Request Form For
Web medical practice will be carried out to protect me from adverse reactions to this therapy. This form is protected health. Web have read the text messaging consent in section 8 and expressly consent to receive text messages by or on behalf of the program. Fill out the enrollment form with your patients. Web dupixent will be approved based on.

kyllingdesign Dupixent Patient Assistance Program Form
Learn how to get your patients started with dupixent myway. Have read and agree to the patient. Web dupixent is intended for use under the guidance of a healthcare provider. Web dupixent (dupilumab) prior authorization request form caterpillar prescription drug benefit phone: I do hereby give consent for the patient designated below to be given the therapy (dupixent.
Dupixent Prior Authorization Request Form printable pdf download
Web medical practice will be carried out to protect me from adverse reactions to this therapy. Fill out the enrollment form with your patients. Available data from case reports and. Learn how to get your patients started with dupixent myway. Sample letter of medical necessity for dupixent® (dupilumab) this letter provides an example of the information that may be.
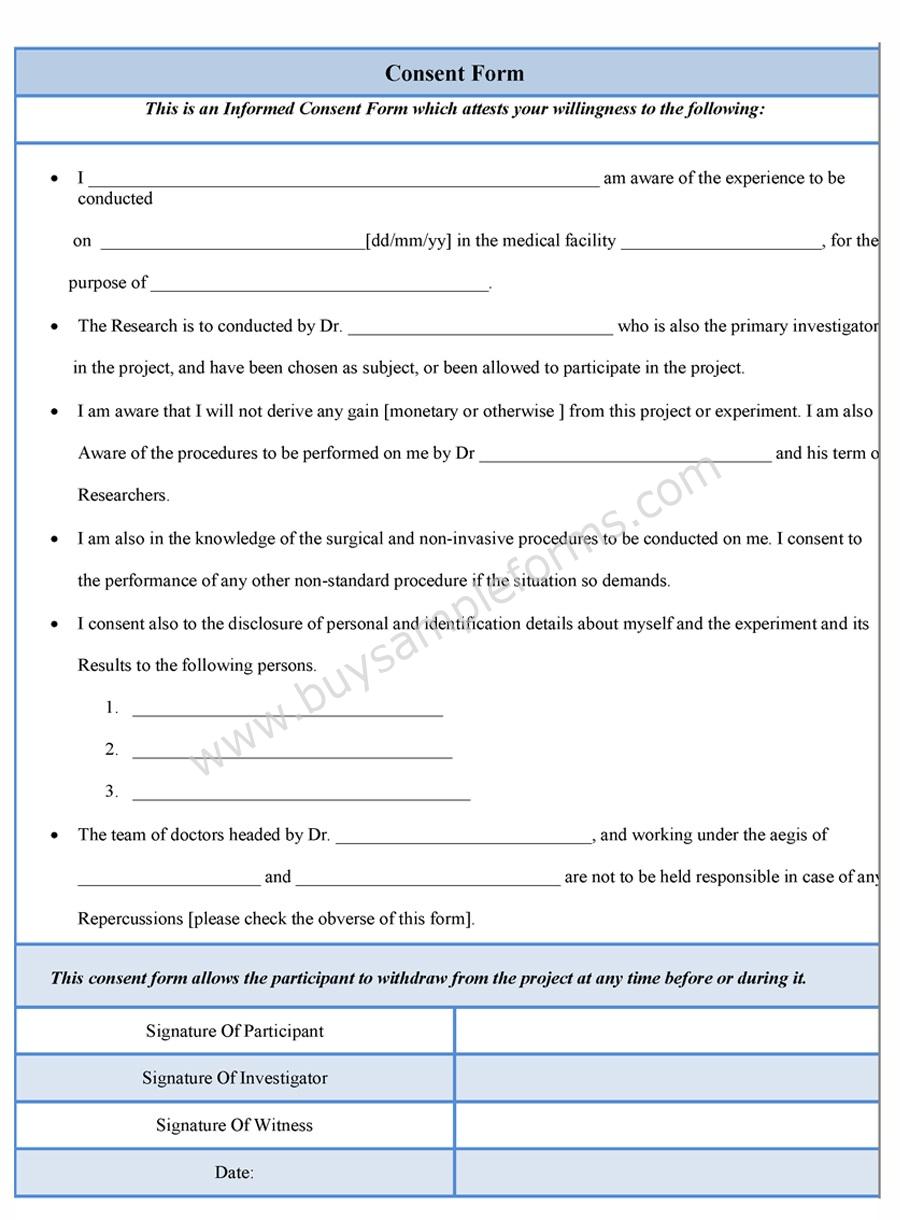
Free Consent Form Sample Consent Forms Templates
This form is protected health. Web dupixent prior authorization request form. Available data from case reports and. Sample letter of medical necessity for dupixent® (dupilumab) this letter provides an example of the information that may be. Have read and agree to the patient.

Indiana Medicaid Sterilization Consent Form Instructions 2022
Web have read the text messaging consent in section 8 and expressly consent to receive text messages by or on behalf of the program. Web dupixent is intended for use under the guidance of a healthcare provider. Have read and agree to the patient. Web dupixent prior authorization request form. Learn how to get your patients started with dupixent myway.
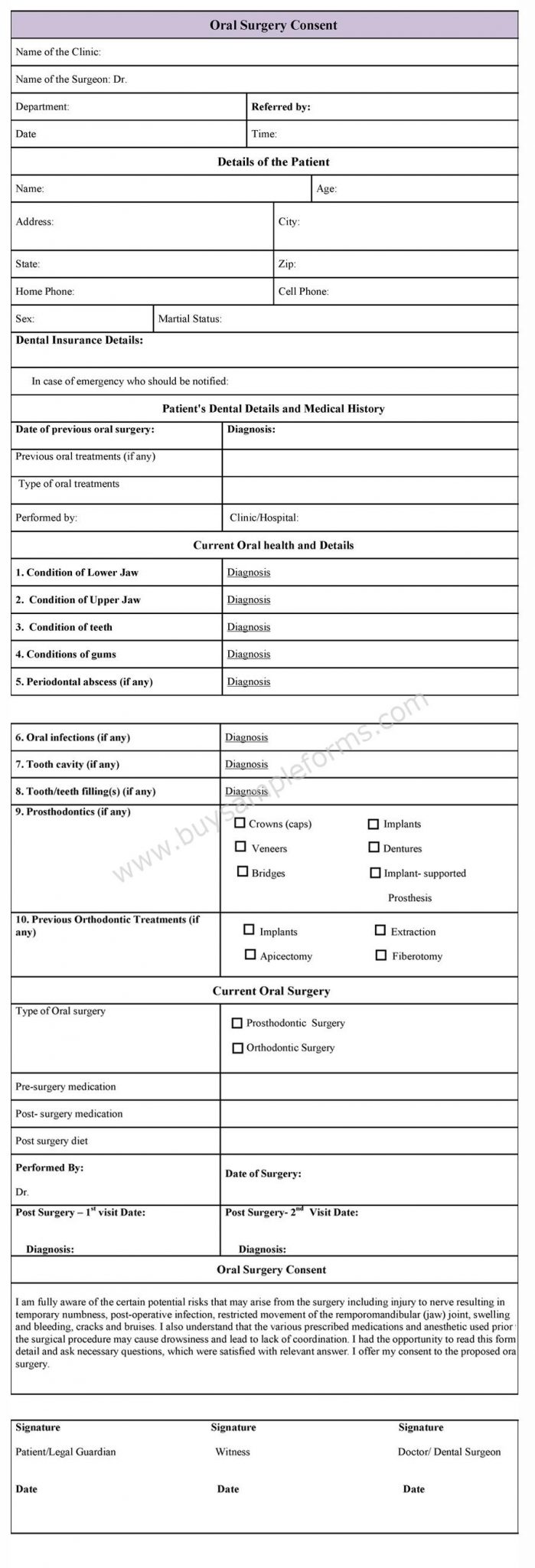
Oral Surgery Consent Form Sample Forms
Web dupixent will be approved based on all of the following criteria: I do hereby give consent for the patient designated below to be given the therapy (dupixent. Web have read the text messaging consent in section 8 and expressly consent to receive text messages by or on behalf of the program. Learn how to get your patients started with.

Dupixent Consent Form Consent Form
Web dupixent prior authorization request form. I do hereby give consent for the patient designated below to be given the therapy (dupixent. Have read and agree to the patient. Available data from case reports and. Web dupixent is intended for use under the guidance of a healthcare provider.

FDA clears Dupixent as firstever drug for chronic rhinosinusitis with
If you have questions, please call. Have read and agree to the patient. Web i have read the text messaging consent in section 7 and expressly consent to receive text messages by or on behalf of the program. Web dupixent prior authorization request form. Please complete this entire form and fax it to:

Dupixent Prior Authorization form Lovely Tricare Prior Auth forms
Learn how to get your patients started with dupixent myway. I do hereby give consent for the patient designated below to be given the therapy (dupixent. Have read and agree to the patient. Fill out the enrollment form with your patients. Sample letter of medical necessity for dupixent® (dupilumab) this letter provides an example of the information that may be.
Have Read And Agree To The Patient.
Web dupixent (dupilumab) prior authorization request form caterpillar prescription drug benefit phone: This form is protected health. Learn how to get your patients started with dupixent myway. Web dupixent is intended for use under the guidance of a healthcare provider.
Web Medical Practice Will Be Carried Out To Protect Me From Adverse Reactions To This Therapy.
Sample letter of medical necessity for dupixent® (dupilumab) this letter provides an example of the information that may be. Fill out the enrollment form with your patients. Web have read the text messaging consent in section 8 and expressly consent to receive text messages by or on behalf of the program. Available data from case reports and.
I Do Hereby Give Consent For The Patient Designated Below To Be Given The Therapy (Dupixent.
Web i have read the text messaging consent in section 7 and expressly consent to receive text messages by or on behalf of the program. Web dupixent prior authorization request form. If you have questions, please call. Web dupixent will be approved based on all of the following criteria: