Example Cms 1500 Form
Example Cms 1500 Form - This is a sample only. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. You can decide how often to. Please adapt to your billing situation. You'll see instructions on how to complete the field. This form is the only version accepted by medicare. Sign up to get the latest information about your choice of cms topics. Always use pica or arial fonts to fill out these forms. (for example, see application number hcp220517faenj). Insured’s policy group or feca number a.
The form is used by physicians and allied health professionals to submit claims for medical services. Refer to the surgery sections of this manual for detailed policy information. This interactive guide provides instruction on how to complete the form. Web cms 1500 dynamic list information. Do not use italics or broken characters, dot matrix fonts, stylized fonts, or red ink when filling. Cms generally creates codes for products themselves, without specifying a route of administration. This is a sample only. Enter the acquisition cost for pharmaceutical or radiopharmaceutical diagnostic imaging agents or for therapeutic radionuclides. Always use pica or arial fonts to fill out these forms. This form is the only version accepted by medicare.
This form is the only version accepted by medicare. The form is used by physicians and allied health professionals to submit claims for medical services. The cms 1500 form is only filed by health care providers or medical suppliers, not by patients. The form is published by the centers for medicare and medicaid services. This interactive guide provides instruction on how to complete the form. The font size is between 10 and 12. You'll see instructions on how to complete the field. Information collected on this form includes basic. Web the following tips will help you fill out cms 1500 successfully and accurately: It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services.
:max_bytes(150000):strip_icc()/CMS-1500-claim-form-57a2d3a85f9b589aa99caf8b.jpg)
CMS 1500 Claim Form Versions and Tips
(for example, see application number hcp220517faenj). Please adapt to your billing situation. You'll see instructions on how to complete the field. The patient was seen for an office visit. Insured’s name (last name, first name, middle initial) 7.
New CMS1500 Form (02/12) YouTube
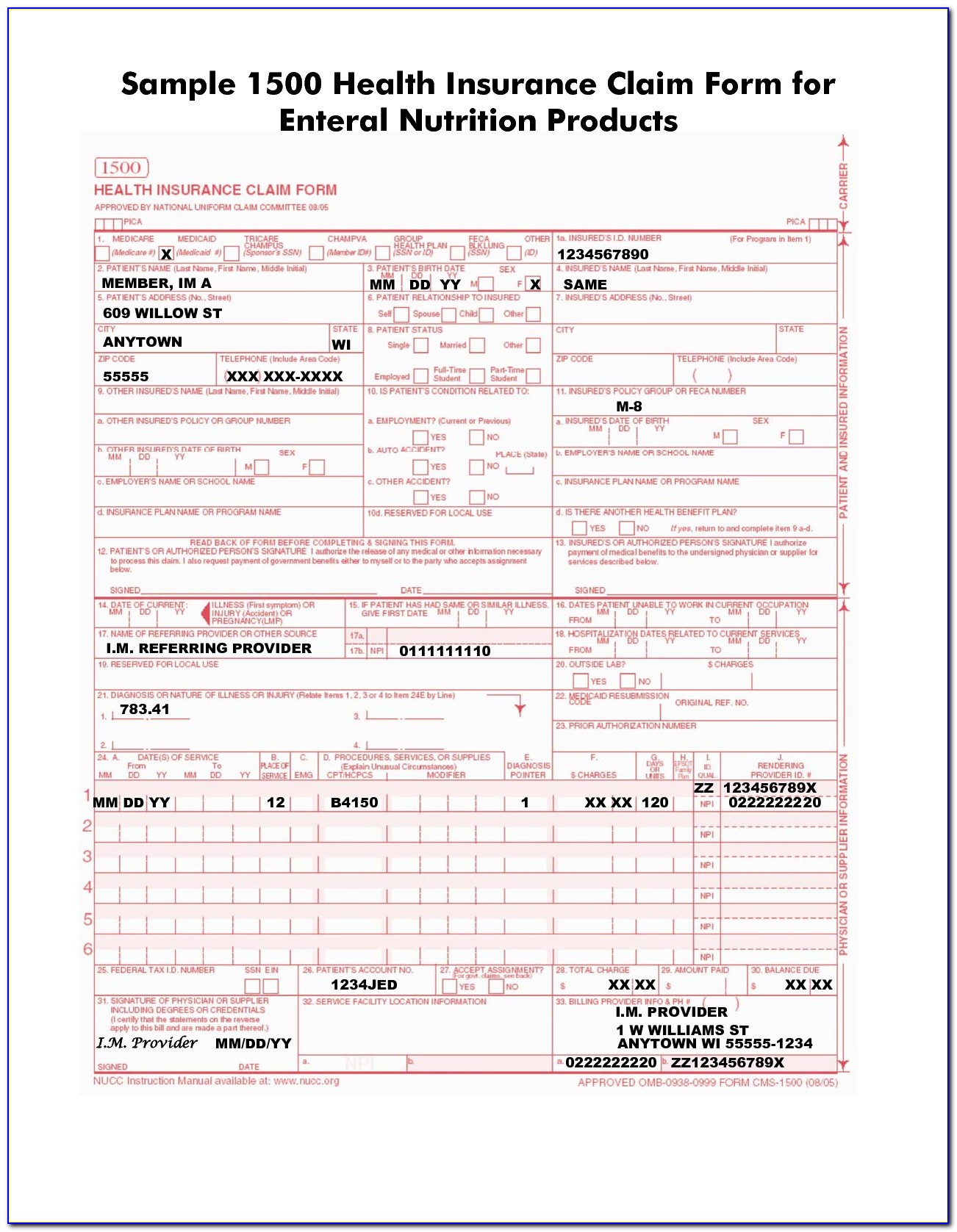
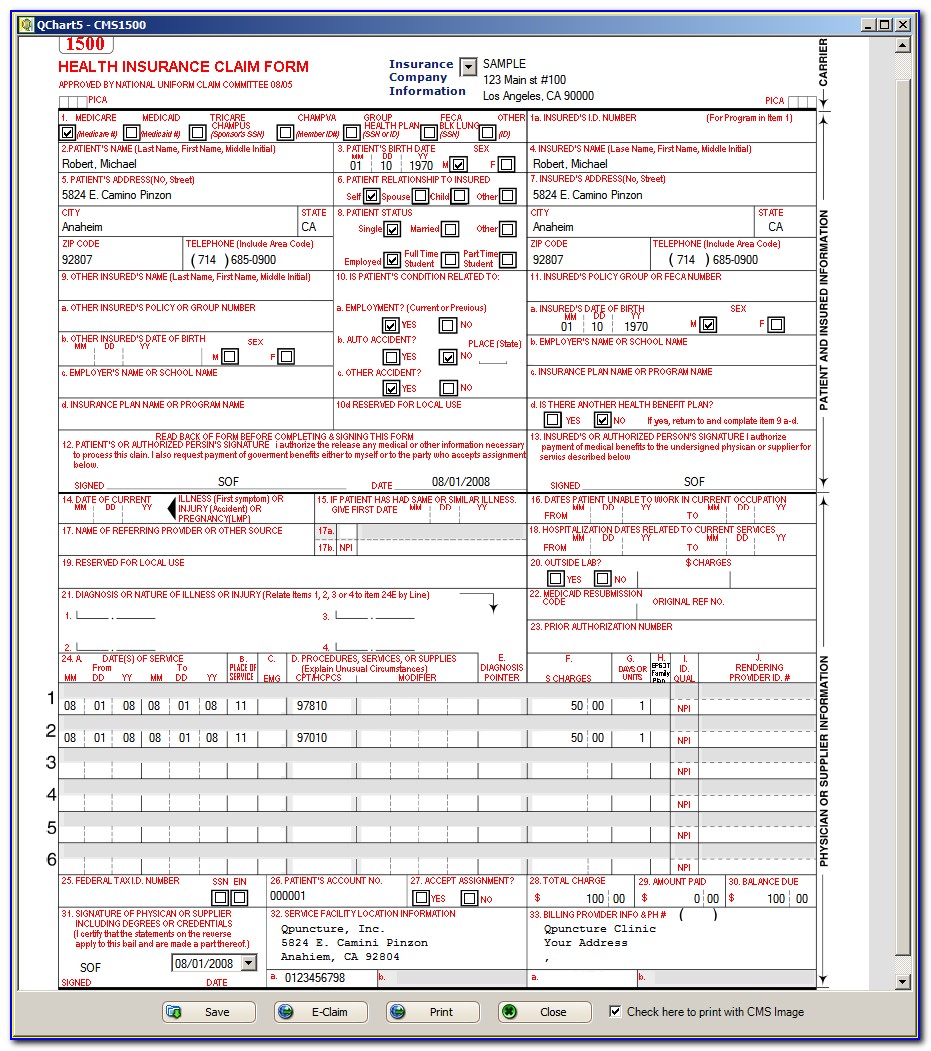
The patient was seen for an office visit. The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. Refer to the surgery sections of this manual for detailed policy information. Web health insurance claim form approved by national uniform claim committee omb no. Web the following tips will help you fill out.
cms claimbilling CMS 1500 claim form billing instruction Part 2
Web the cms 1500 form is a claim form used by health care providers to file for payment of medicare and medicaid claims. Fill the form with capital letters and always use black ink or black fonts. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Web cms 1500 dynamic list information..

Cms 1500 Claim Form Instructions 2016 Form Resume Examples XE8je6e3Oo
This form is the only version accepted by medicare. Insured’s name (last name, first name, middle initial) 7. Insured’s address (no., street) city state zip code telephone (include area code) 11. Number (for program in item 1) 4. Billing various government and some private insurers.
Cms 1500 Claim Form Instructions When Medicare Is Secondary Form
You'll see instructions on how to complete the field. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Insured’s policy group or feca number a. Web health insurance claim form.

Example Of Cms 1500 Form Completed with Cms 1500 Form Free Medical
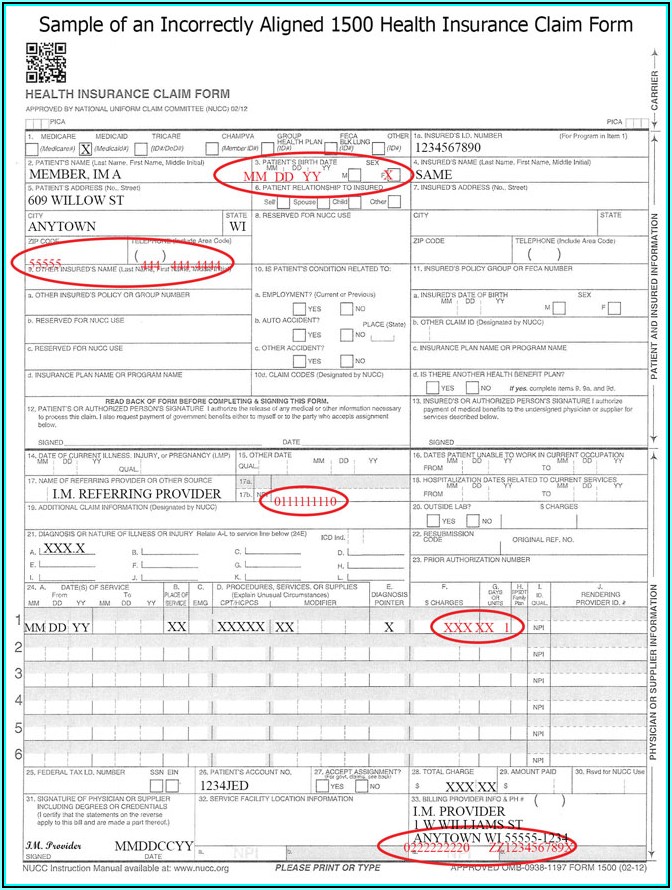
Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy. Fill the form with capital letters and always use black ink or black fonts. Please adapt to your billing situation. Sign up to get the latest information about your choice of cms topics. The center of medicaid and medicare services (cms).
Example Hcfa 1500 Form Filled Out Form Resume Examples qQ5MNjdOXg
Refer to the surgery sections of this manual for detailed policy information. This interactive guide provides instruction on how to complete the form. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Always use pica or arial fonts to fill out these forms. Web the cms 1500 form is a claim form.

Sample Cms 1500 Form Filled Out Form Resume Examples 05KA75m8wP
Please adapt to your billing situation. Billing example for weekly injections. The first injection is administered on august 10, 2014 and the second injection is administered on august 17, 2014. The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. Claims may be electronically submitted to a medicare carrier, durable medical equipment.
Medicare Cms 1500 Claim Form Form Resume Examples v19xkPk27E
You can decide how often to. Do not use italics or broken characters, dot matrix fonts, stylized fonts, or red ink when filling. Insured’s name (last name, first name, middle initial) 7. (for example, see application number hcp220517faenj). Fill the form with capital letters and always use black ink or black fonts.

Sample Cms 1500 Form Filled Out Form Resume Examples 05KA75m8wP
Enter the acquisition cost for pharmaceutical or radiopharmaceutical diagnostic imaging agents or for therapeutic radionuclides. This is a sample only. The font size is between 10 and 12. The center of medicaid and medicare services (cms) form 1500 is used to bill sfhp for medical services. Please adapt to your billing situation.
Billing Various Government And Some Private Insurers.
Do not use italics or broken characters, dot matrix fonts, stylized fonts, or red ink when filling. The cms 1500 form is only filed by health care providers or medical suppliers, not by patients. You'll see instructions on how to complete the field. Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy.
(For Example, See Application Number Hcp220517Faenj).
The form is published by the centers for medicare and medicaid services. Number (for program in item 1) 4. Enter the acquisition cost for pharmaceutical or radiopharmaceutical diagnostic imaging agents or for therapeutic radionuclides. Insured’s policy group or feca number a.
The Font Size Is Between 10 And 12.
Fill the form with capital letters and always use black ink or black fonts. The form is used by physicians and allied health professionals to submit claims for medical services. Cms generally creates codes for products themselves, without specifying a route of administration. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers.
This Form Is The Only Version Accepted By Medicare.
Web cms 1500 dynamic list information. Web health insurance claim form approved by national uniform claim committee omb no. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Insured’s name (last name, first name, middle initial) 7.