Hcas Provider Enrollment Form
Hcas Provider Enrollment Form - • health plan contracting and enrollment required documents list. Street city state zip code email telephone fax contact name optional practice information office hours: • enrollment and credentialing application status inquiries. • sample hcas reference letter. Ancillary contracting and credentialing application form; • hcas hospital roster submission process. Ancillary practitioner data form behavioral health Web hcas provider enrollment form date completed by telephone email of person completing form section 1: Involved parties names, addresses and numbers etc. Monday tuesday wednesday thursday friday saturday sunday average waiting time to schedule:
Primary practice information please check box to indicate address type. Monday tuesday wednesday thursday friday saturday sunday average waiting time to schedule: Use last page to list additional addresses. Web resource center commercial forms from filing an appeal to requesting authorization, from on this page you have access to the forms you’ll need for harvard pilgrim’s commercial line of business. Includes ambulance, asc, dme, home care, laboratories, radiology, snfs, and urgent care. Involved parties names, addresses and numbers etc. • enrollment and credentialing application status inquiries. Add the day/time and place your electronic signature. • health plan contracting and enrollment required documents list. Web hcas provider enrollment form optional practice information office hours monday tuesday wednesday average waiting time to schedule:
Web resource center commercial forms from filing an appeal to requesting authorization, from on this page you have access to the forms you’ll need for harvard pilgrim’s commercial line of business. Web hcas provider enrollment form. Please complete a separate page for all new enrollees in the group. Street city state zip code email telephone fax contact name optional practice information office hours: Add the day/time and place your electronic signature. Web get the hcas form 2020 you need. Ancillary contracting and credentialing application form; Ancillary practitioner data form behavioral health Includes ambulance, asc, dme, home care, laboratories, radiology, snfs, and urgent care. Primary practice information please check box to indicate address type.
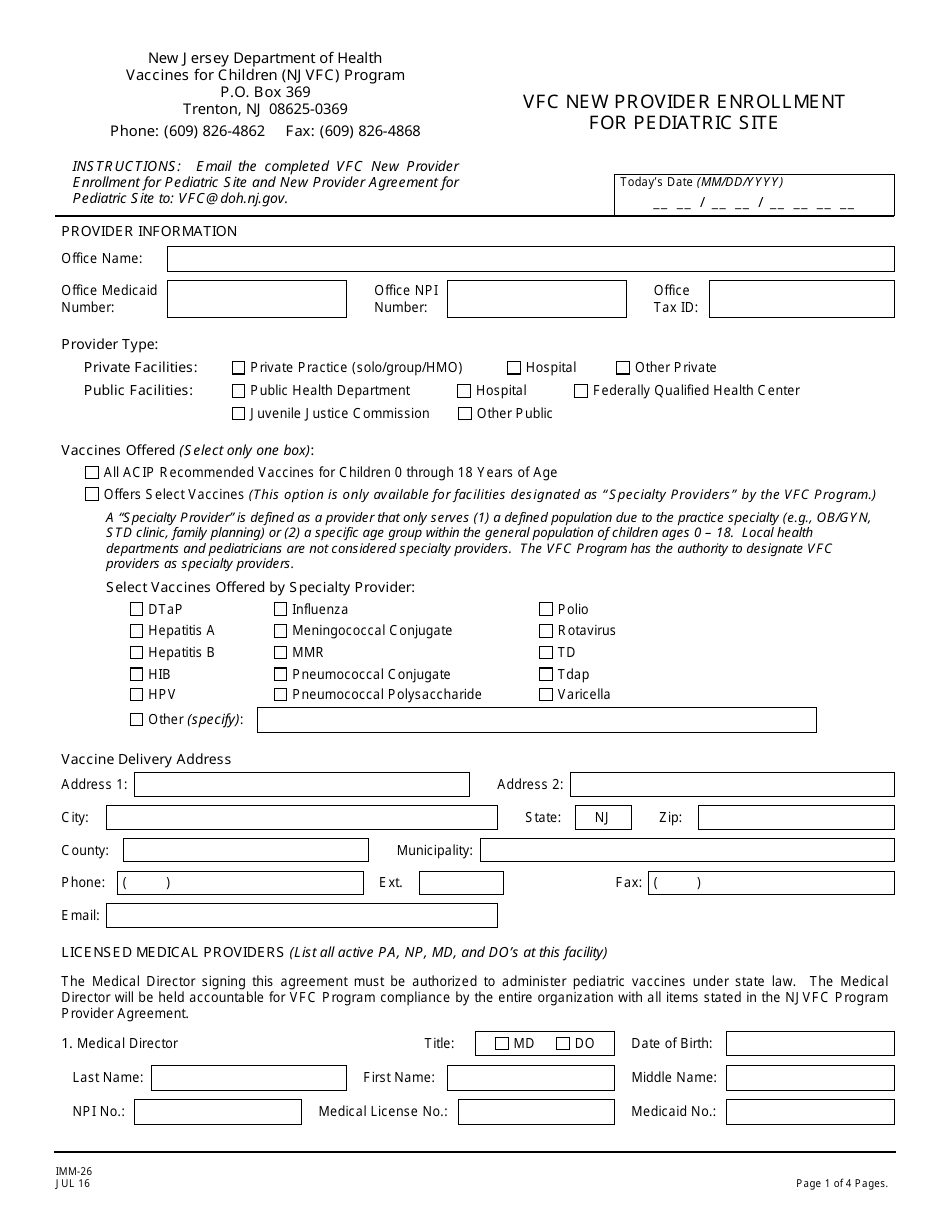
Form IMM26 Download Printable PDF or Fill Online Vfc New Provider
Web hcas provider enrollment form; • enrollment and credentialing application status inquiries. Use last page to list additional addresses. • health plan contracting and enrollment required documents list. Add the day/time and place your electronic signature.
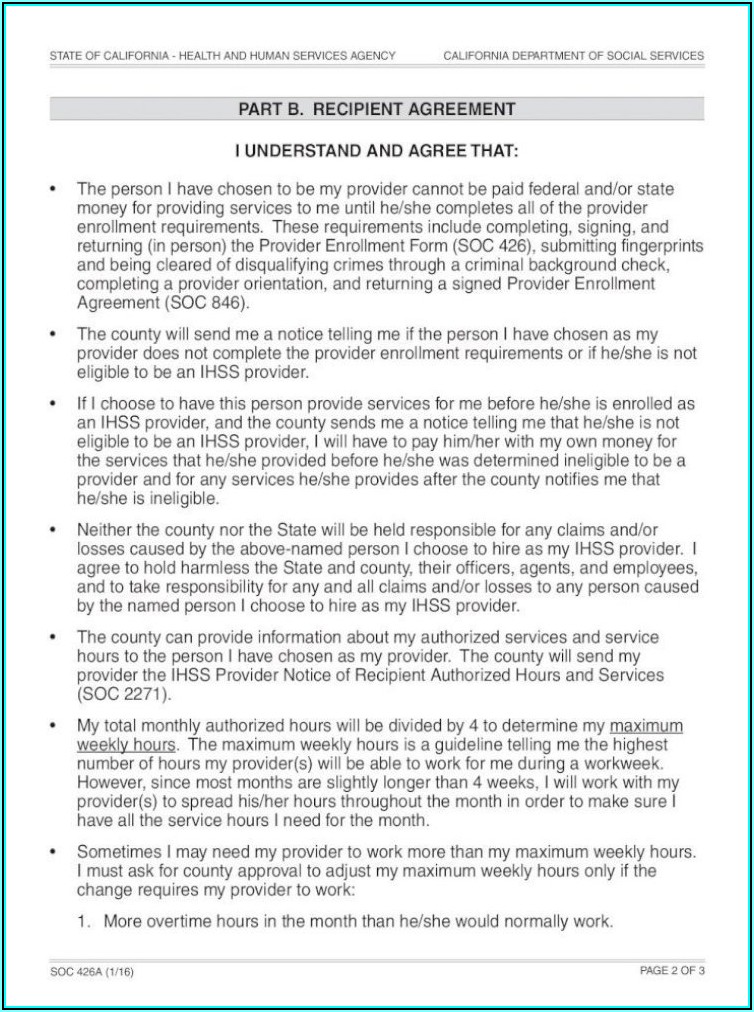
Ihss Provider Enrollment Agreement Form Form Resume Examples
Primary practice information please check box to indicate address type. Customize the blanks with exclusive fillable fields. • hcas hospital roster submission process. Please complete a separate page for all new enrollees in the group. Includes ambulance, asc, dme, home care, laboratories, radiology, snfs, and urgent care.

Provider Enrollment Apple Billing And Credentialing
Please complete a separate page for all new enrollees in the group. Monday tuesday wednesday thursday friday saturday sunday average waiting time to schedule: Involved parties names, addresses and numbers etc. • sample hcas reference letter. Web hcas provider enrollment form optional practice information office hours monday tuesday wednesday average waiting time to schedule:
32bjfunds Enrollment Form Enrollment Form
Web hcas provider enrollment form optional practice information office hours monday tuesday wednesday average waiting time to schedule: • sample hcas reference letter. Web resource center commercial forms from filing an appeal to requesting authorization, from on this page you have access to the forms you’ll need for harvard pilgrim’s commercial line of business. • health plan contracting and enrollment.
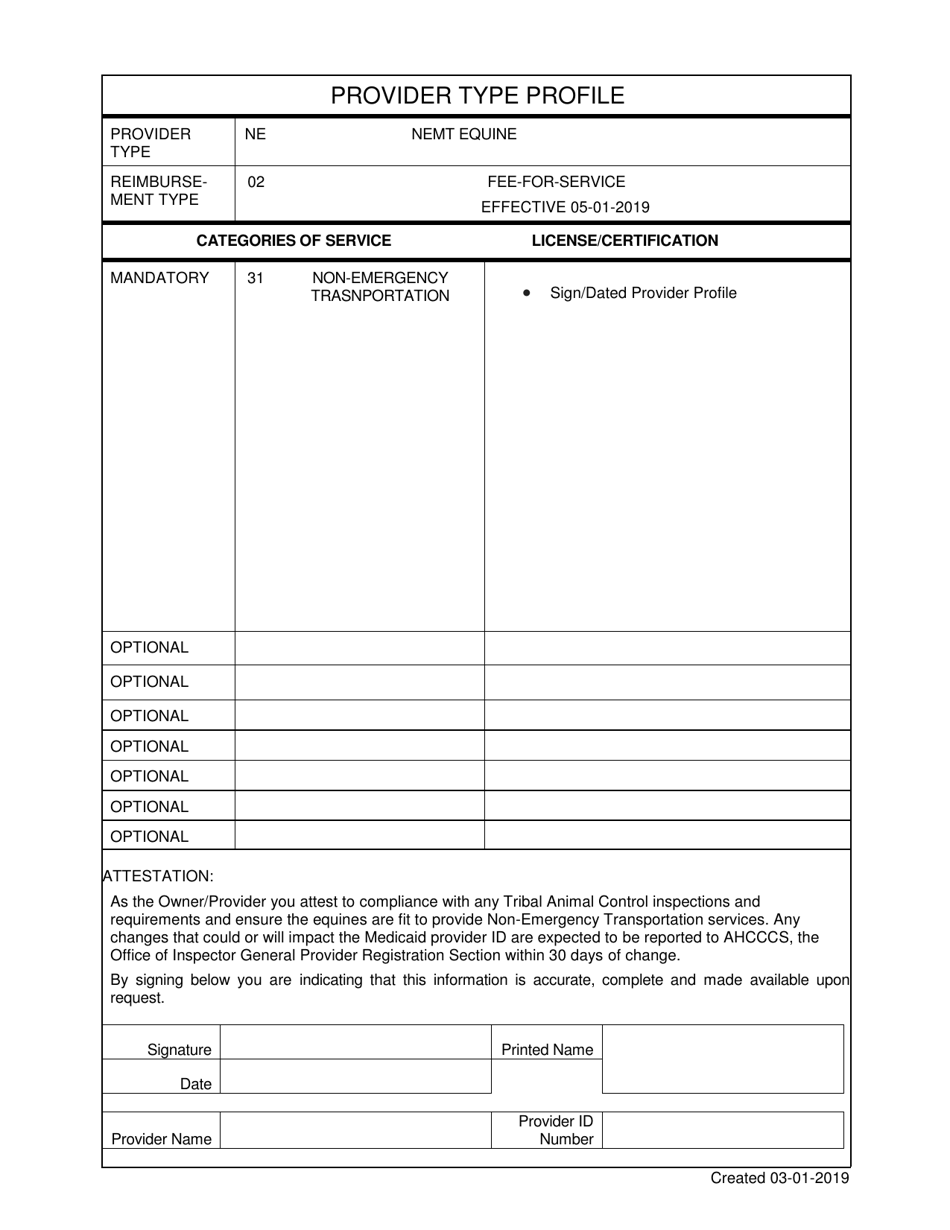
Arizona Provider Enrollment Application Nemt Equine Download Fillable
Web resource center commercial forms from filing an appeal to requesting authorization, from on this page you have access to the forms you’ll need for harvard pilgrim’s commercial line of business. Ancillary services letter of intent; • sample hcas reference letter. Ancillary contracting and credentialing application form; Includes ambulance, asc, dme, home care, laboratories, radiology, snfs, and urgent care.

Verityhealth Fill Online, Printable, Fillable, Blank pdfFiller
• hcas hospital roster submission process. Primary practice information please check box to indicate address type. Customize the blanks with exclusive fillable fields. Web hcas provider enrollment form. Web resource center commercial forms from filing an appeal to requesting authorization, from on this page you have access to the forms you’ll need for harvard pilgrim’s commercial line of business.
Aarp Provider Enrollment Form Form Resume Examples xg5bQljDlY
• hcas provider enrollment form (ms word) • integrated massachusetts application. Monday tuesday wednesday thursday friday saturday sunday average waiting time to schedule: Ancillary services letter of intent; Tax identification number group npi # payment address. • health plan contracting and enrollment required documents list.
HCAS Provider Enrollment Form
Street city state zip code email telephone fax contact name optional practice information office hours: Tax identification number group npi # payment address. Customize the blanks with exclusive fillable fields. Web hcas provider enrollment form date completed by telephone email of person completing form section 1: Web hcas provider enrollment form.
HCAS Provider Enrollment Form
Street city state zip code email telephone fax contact name optional practice information office hours: Tax identification number group npi # payment address. Involved parties names, addresses and numbers etc. • hcas provider enrollment form (ms word) • integrated massachusetts application. • health plan contracting and enrollment required documents list.
National Provider Enrollment Conference 2021 Fill Out and Sign
Monday tuesday wednesday thursday friday saturday sunday average waiting time to schedule: Web resource center commercial forms from filing an appeal to requesting authorization, from on this page you have access to the forms you’ll need for harvard pilgrim’s commercial line of business. Involved parties names, addresses and numbers etc. Thursday friday saturday sunday initial visit routine physical covering physicians.
Street City State Zip Code Email Telephone Fax Contact Name Optional Practice Information Office Hours:
• enrollment and credentialing application status inquiries. Web get the hcas form 2020 you need. • sample hcas reference letter. • hcas provider enrollment form (ms word) • integrated massachusetts application.
Web Hcas Provider Enrollment Form.
Primary practice information please check box to indicate address type. Use last page to list additional addresses. Customize the blanks with exclusive fillable fields. Add the day/time and place your electronic signature.
Ancillary Practitioner Data Form Behavioral Health
Web hcas provider enrollment form; Monday tuesday wednesday thursday friday saturday sunday average waiting time to schedule: Involved parties names, addresses and numbers etc. Ancillary contracting and credentialing application form;
Ancillary Services Letter Of Intent;
• health plan contracting and enrollment required documents list. Web providers are enrolled in harvard pilgrim’s provider database consistent with their national provider identifier (npi) and business relationships they establish with facilities, organizations, and clinicians included in the harvard pilgrim network. Thursday friday saturday sunday initial visit routine physical covering physicians (attach additional sheet if necessary) name specialty urgent visit provider type phone number Web hcas provider enrollment form date completed by telephone email of person completing form section 1: