Hipaa 1500 Form
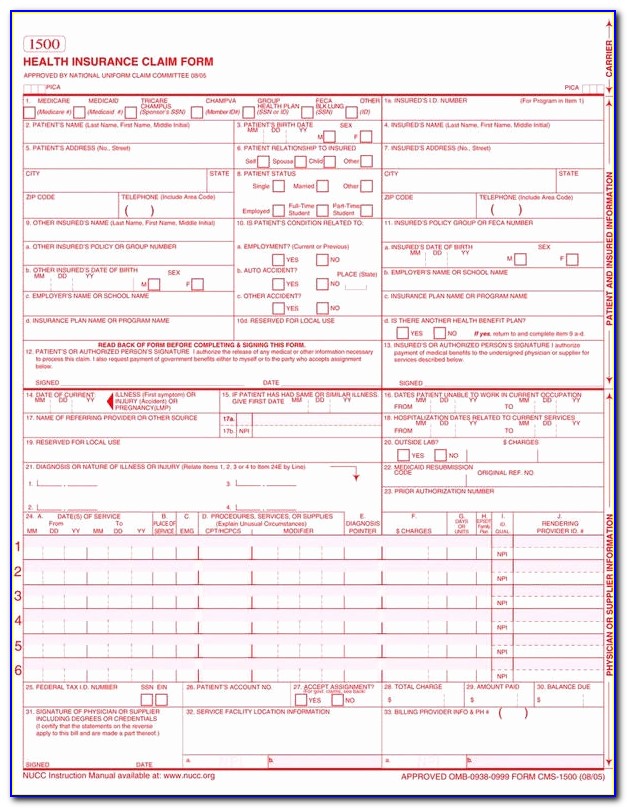
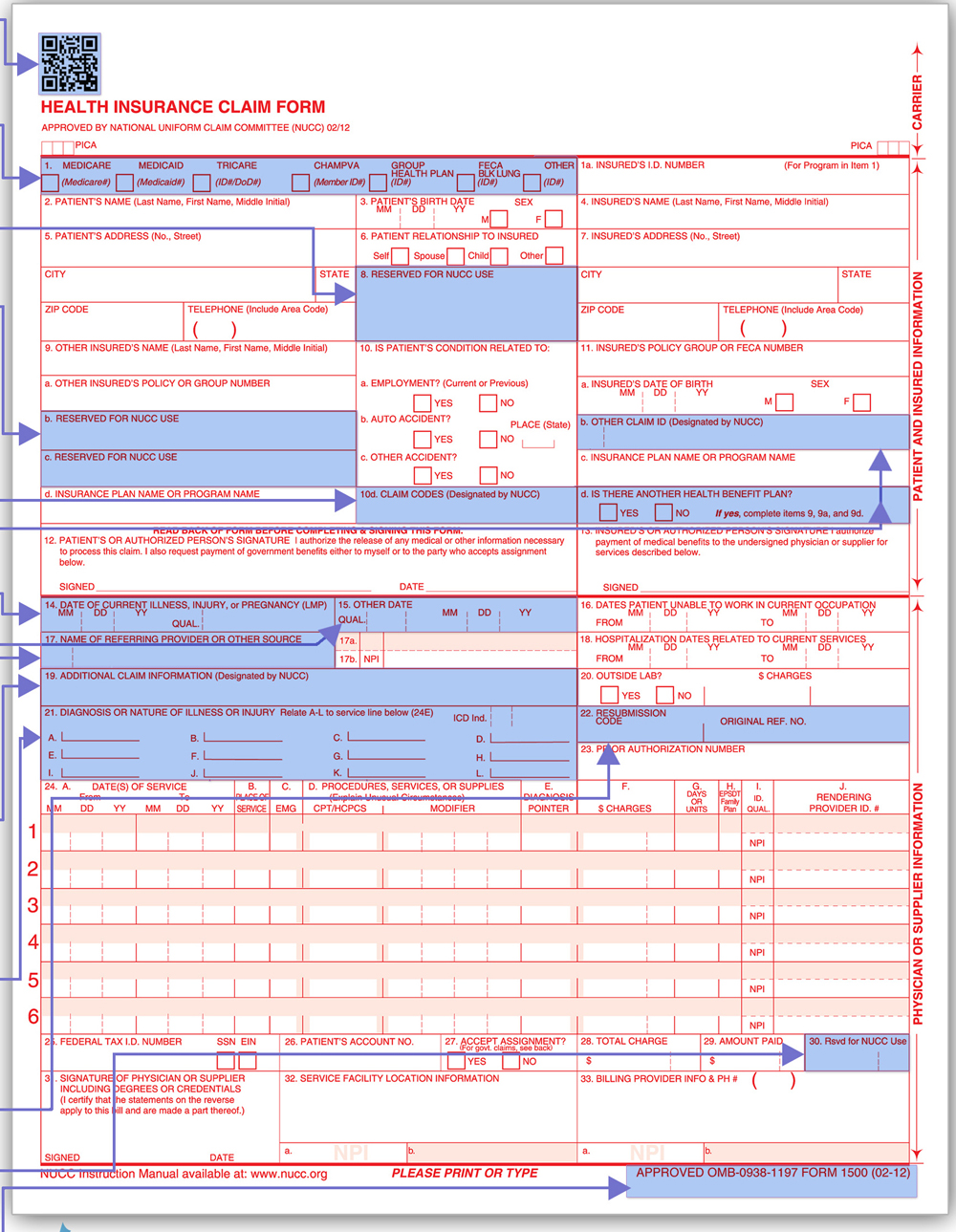
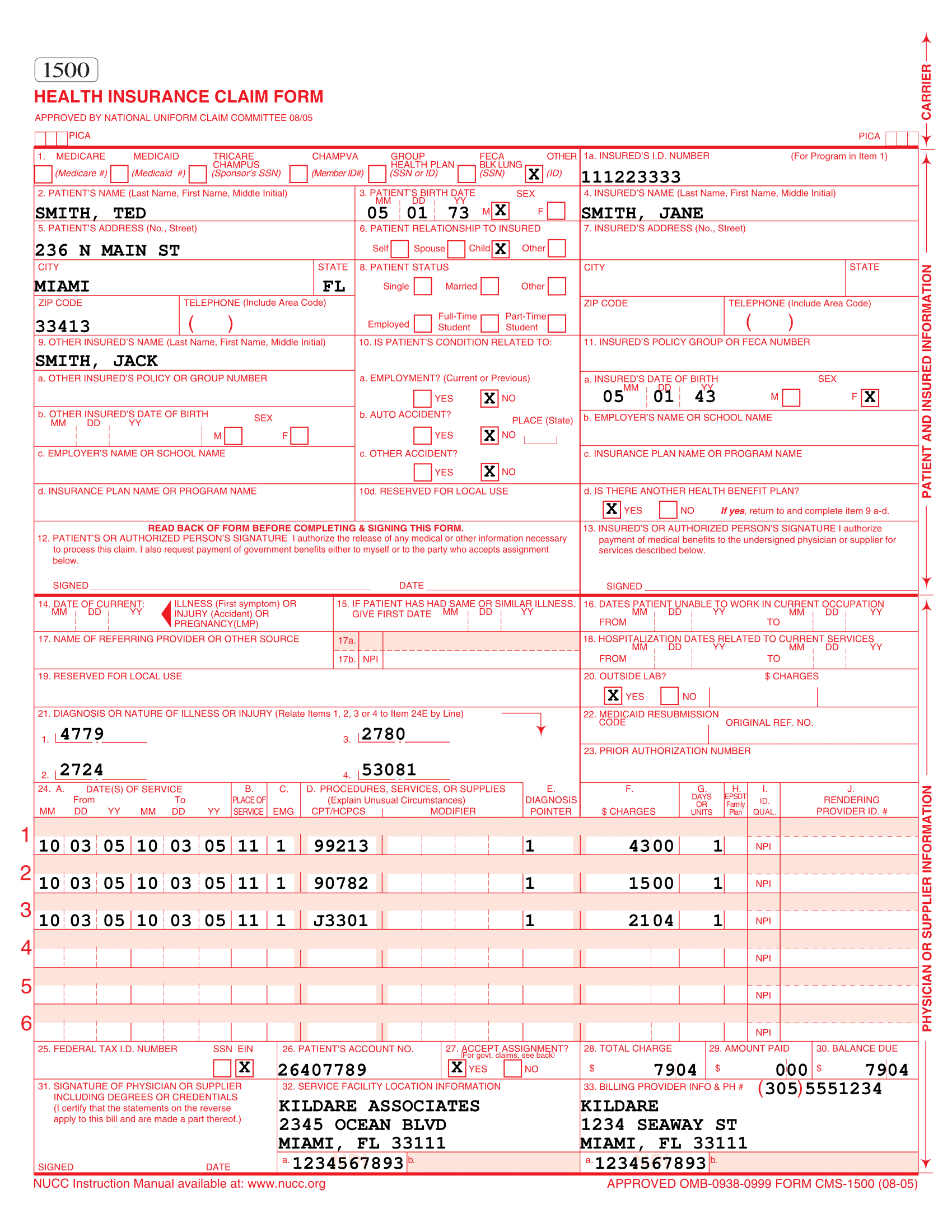
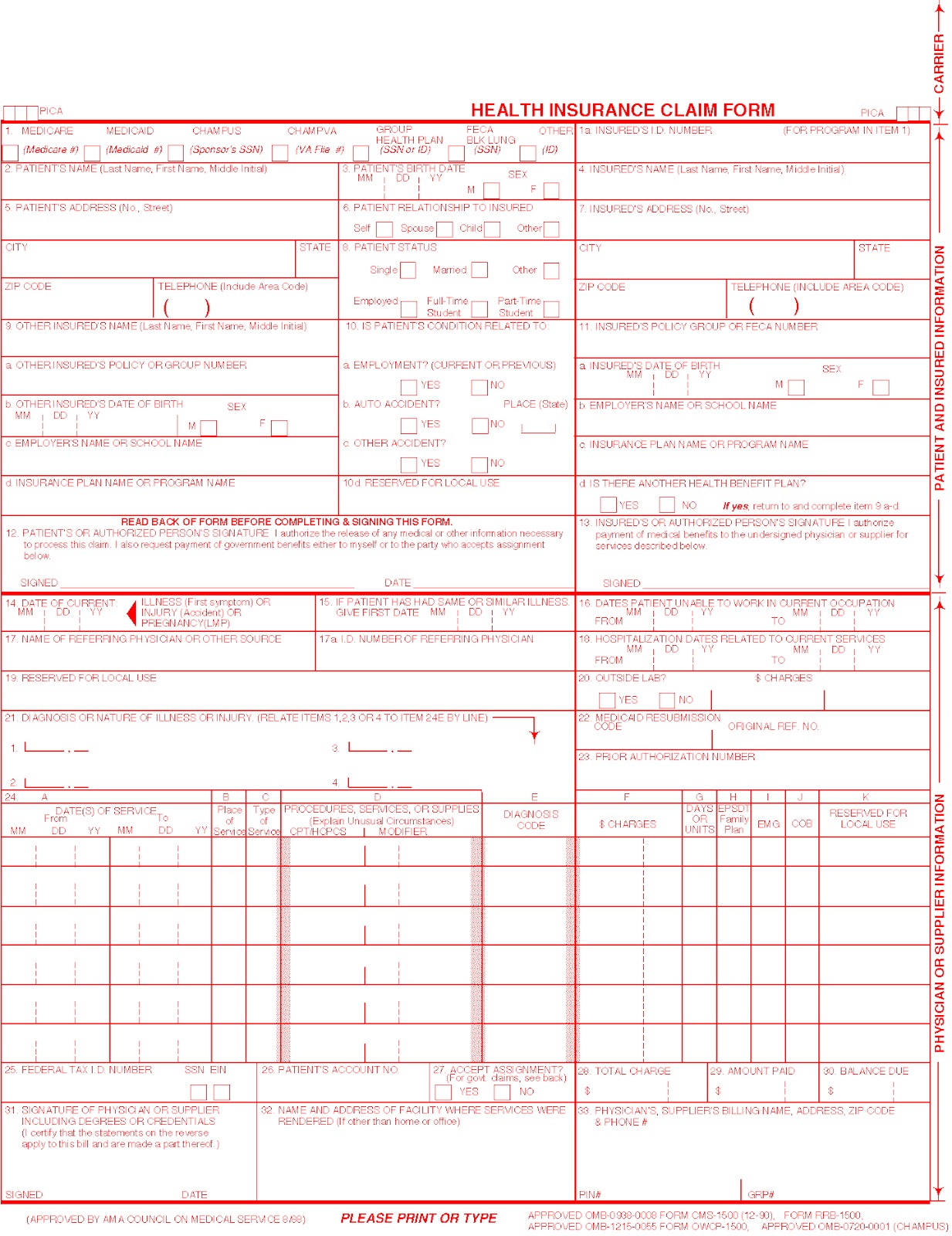
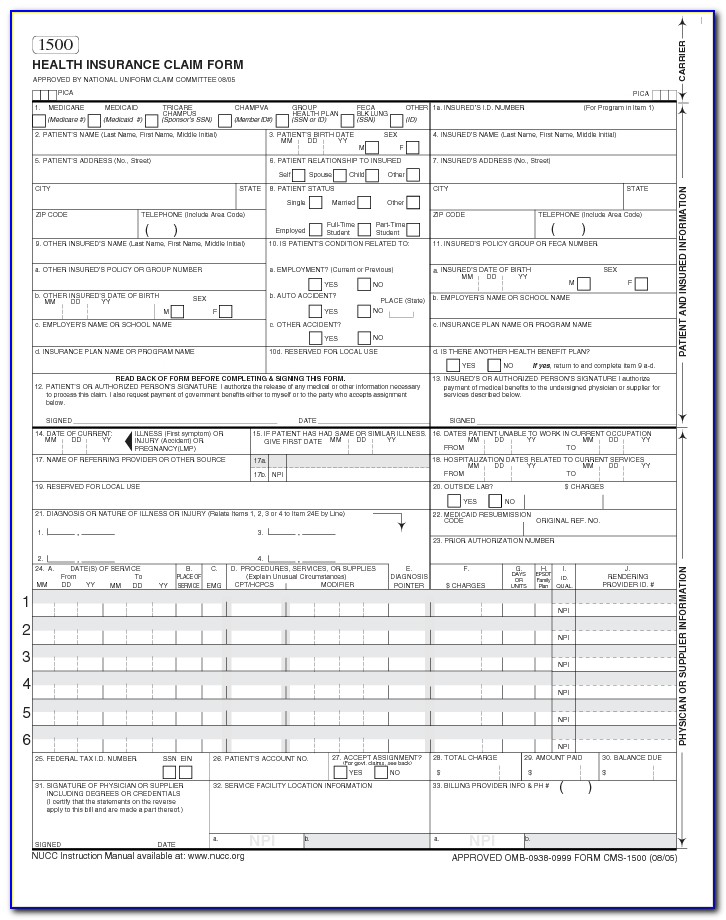
Hipaa 1500 Form - The hcfa 1500/cms claim forms are required for billing insurance purposes, medicare, and federal insurance. Number (for program in item 1) 4. Sign online button or tick the preview image of the blank. The organization responsible for claim content is. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. To start the document, utilize the fill camp; Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. Insured’s address (no., street) city state zip code telephone (include area code). The advanced tools of the editor will guide you through the editable pdf template. Enter your official contact and identification details.
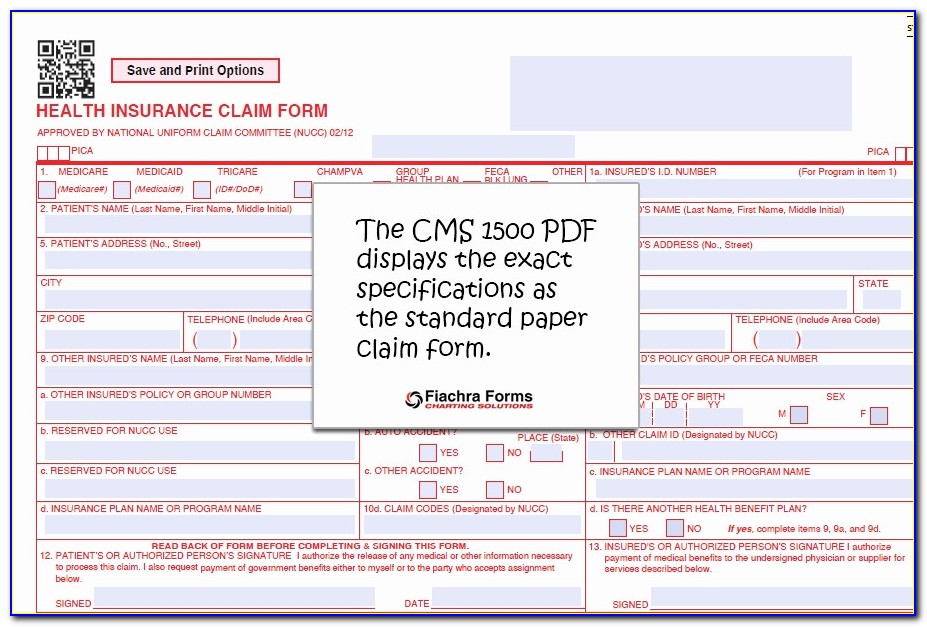
It can be purchased in any version required by calling the u.s. Web tips on how to fill out the hevalth claim form 1500 on the internet: At filerx.com, our cms/hcfa 1500 forms are fully. Insured’s address (no., street) city state zip code telephone (include area code). This document provides information on submitting cms form 1500, professional paper claim form. To start the document, utilize the fill camp; Read back of form before completing & signing this form. Centers for medicare & medicaid services (cms) issue date: The advanced tools of the editor will guide you through the editable pdf template. Number (for program in item 1) 4.
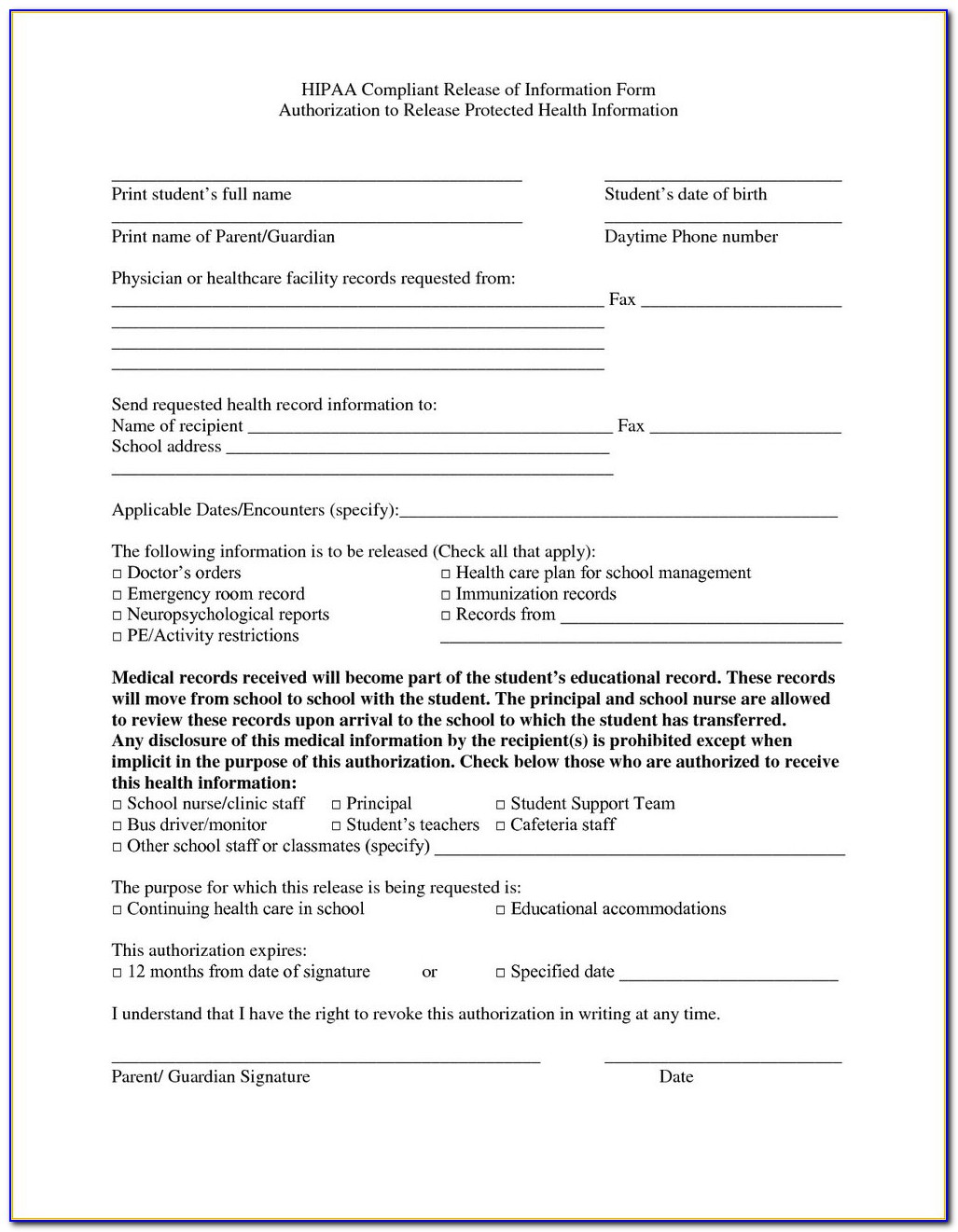
Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. To start the document, utilize the fill camp; Web laser cms/hcfa 1500 forms. Number (for program in item 1) 4. Enter your official contact and identification details. It can be purchased in any version required by calling the u.s. Insured’s address (no., street) city state zip code telephone (include area code). Sign online button or tick the preview image of the blank. Web hipaa for individuals. The organization responsible for claim content is.
Hipaa 1500 Form Pdf Form Resume Examples B8DVGpa5mb
It can be purchased in any version required by calling the u.s. Web tips on how to fill out the hevalth claim form 1500 on the internet: Insured’s address (no., street) city state zip code telephone (include area code). The advanced tools of the editor will guide you through the editable pdf template. Learn your rights under hipaa, how your.
What is the HCFA 1500 form?
Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. The organization responsible for claim content is. At filerx.com, our cms/hcfa 1500 forms are fully in compliance with all government standards, and we guarantee the lowest price in the nation on these forms. Web.
Hipaa 1500 Form Pdf Form Resume Examples B8DVGpa5mb
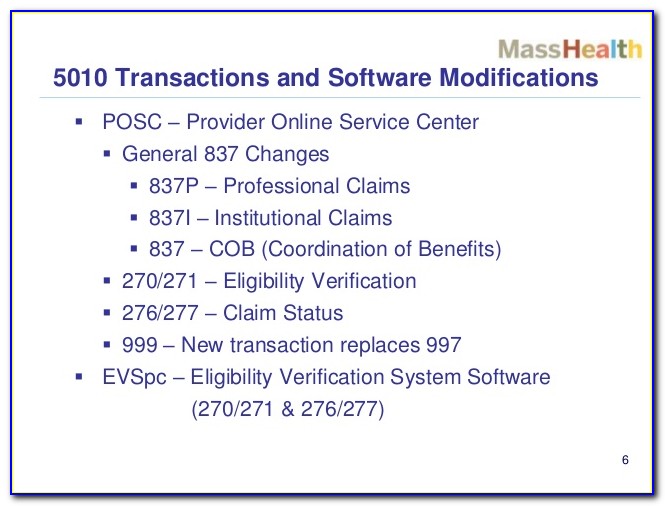
Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Insured’s name (last name, first name, middle initial) 7. Read back of form before completing & signing this form. Web tips.
Hipaa 1500 Form Pdf Form Resume Examples B8DVGpa5mb
Insured’s address (no., street) city state zip code telephone (include area code). Read back of form before completing & signing this form. At filerx.com, our cms/hcfa 1500 forms are fully in compliance with all government standards, and we guarantee the lowest price in the nation on these forms. Web the electronic hipaa claim is based on the _____, which is.
HIPAA 837 professional conversion to CMS 1500 Redix on HIPAA and FHIR
At filerx.com, our cms/hcfa 1500 forms are fully in compliance with all government standards, and we guarantee the lowest price in the nation on these forms. This document provides information on submitting cms form 1500, professional paper claim form. The organization responsible for claim content is. Insured’s address (no., street) city state zip code telephone (include area code). Claims may.
Understanding Your Medical Claims INSURANCE CLAIM FORMS, aka the HCFA1500
To start the document, utilize the fill camp; Sign online button or tick the preview image of the blank. Enter your official contact and identification details. Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. The hcfa 1500/cms claim forms are required for.
Hipaa 1500 Form Pdf Form Resume Examples B8DVGpa5mb
It can be purchased in any version required by calling the u.s. Web hipaa for individuals. Sign online button or tick the preview image of the blank. The advanced tools of the editor will guide you through the editable pdf template. At filerx.com, our cms/hcfa 1500 forms are fully in compliance with all government standards, and we guarantee the lowest.

HIPAA 837 professional conversion to CMS 1500 Redix on HIPAA and FHIR
Insured’s name (last name, first name, middle initial) 7. Centers for medicare & medicaid services (cms) issue date: This document provides information on submitting cms form 1500, professional paper claim form. Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. Read back of.
Hipaa 1500 Form Pdf Form Resume Examples B8DVGpa5mb
Insured’s address (no., street) city state zip code telephone (include area code). At filerx.com, our cms/hcfa 1500 forms are fully. Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. The hcfa 1500/cms claim forms are required for billing insurance purposes, medicare, and federal.
Sample Cms 1500 Form Filled Out Form Resume Examples 05KA75m8wP
Web hipaa for individuals. Sign online button or tick the preview image of the blank. To start the document, utilize the fill camp; Read back of form before completing & signing this form. At filerx.com, our cms/hcfa 1500 forms are fully in compliance with all government standards, and we guarantee the lowest price in the nation on these forms.
This Document Provides Information On Submitting Cms Form 1500, Professional Paper Claim Form.
It can be purchased in any version required by calling the u.s. To start the document, utilize the fill camp; Web tips on how to fill out the hevalth claim form 1500 on the internet: The hcfa 1500/cms claim forms are required for billing insurance purposes, medicare, and federal insurance.
Insured’s Address (No., Street) City State Zip Code Telephone (Include Area Code).
At filerx.com, our cms/hcfa 1500 forms are fully. Enter your official contact and identification details. The advanced tools of the editor will guide you through the editable pdf template. The organization responsible for claim content is.
At Filerx.com, Our Cms/Hcfa 1500 Forms Are Fully In Compliance With All Government Standards, And We Guarantee The Lowest Price In The Nation On These Forms.
Read back of form before completing & signing this form. Web the electronic hipaa claim is based on the _____, which is a paper claim form. Web hipaa for individuals. Number (for program in item 1) 4.
Centers For Medicare & Medicaid Services (Cms) Issue Date:
Sign online button or tick the preview image of the blank. Web laser cms/hcfa 1500 forms. Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. Insured’s name (last name, first name, middle initial) 7.