Kaiser Account Change Form California
Kaiser Account Change Form California - Web instructions • there are different types of plan changes and account changes you can make with this form. Please fill out your personal information in section a. Web quick access to online forms and documents that help you manage enrollment, certification, and more. Fill out your information if you’re making a change, please update the boxes below with your new information. A.company information company and subscriber information (to be completed. First name mi date of birth (mm/dd/yyyy) last name medical. Web open enrollment has ended. Page 6 of 6 h. Web california region group enrollment/change form please print or type in black ink only. Looking for information about the services we offer?
Web 2 company name change new company name previous company name 3 company address change check here if all addresses are the same new physical street. Please fill out your personal information in section a. See instructions on reverse before completing this form. If required, you'll need to provide proof of your qualifying life event and fill out and send in our proof of qualifying life event. Page 6 of 6 h. First name mi date of birth (mm/dd/yyyy) last name medical. Web open enrollment has ended. Web *603376096* california subscriber enrollment/change form please print in blue or black ink only. A.company information company and subscriber information (to be completed. View, download, or print commonly used forms, guidebooks, handbooks, and other.
View, download, or print commonly used forms, guidebooks, handbooks, and other. Web california region group enrollment/change form please print or type in black ink only. Web open enrollment has ended. Web you can fill out and send in an account change form. First name mi date of birth (mm/dd/yyyy) last name medical. Web 2 company name change new company name previous company name 3 company address change check here if all addresses are the same new physical street. Fill out your information if you’re making a change, please update the boxes below with your new information. Web use this form to make changes to your kaiser permanente child health program / community health care program account, which provides help in paying your health. Make a copy for your records. Page 6 of 6 h.

Helpful Forms USW Local 6787
Please fill out your personal information in section a. Web *603376096* california subscriber enrollment/change form please print in blue or black ink only. Web open enrollment has ended. If required, you'll need to provide proof of your qualifying life event and fill out and send in our proof of qualifying life event. Web complete an account change form (available below).
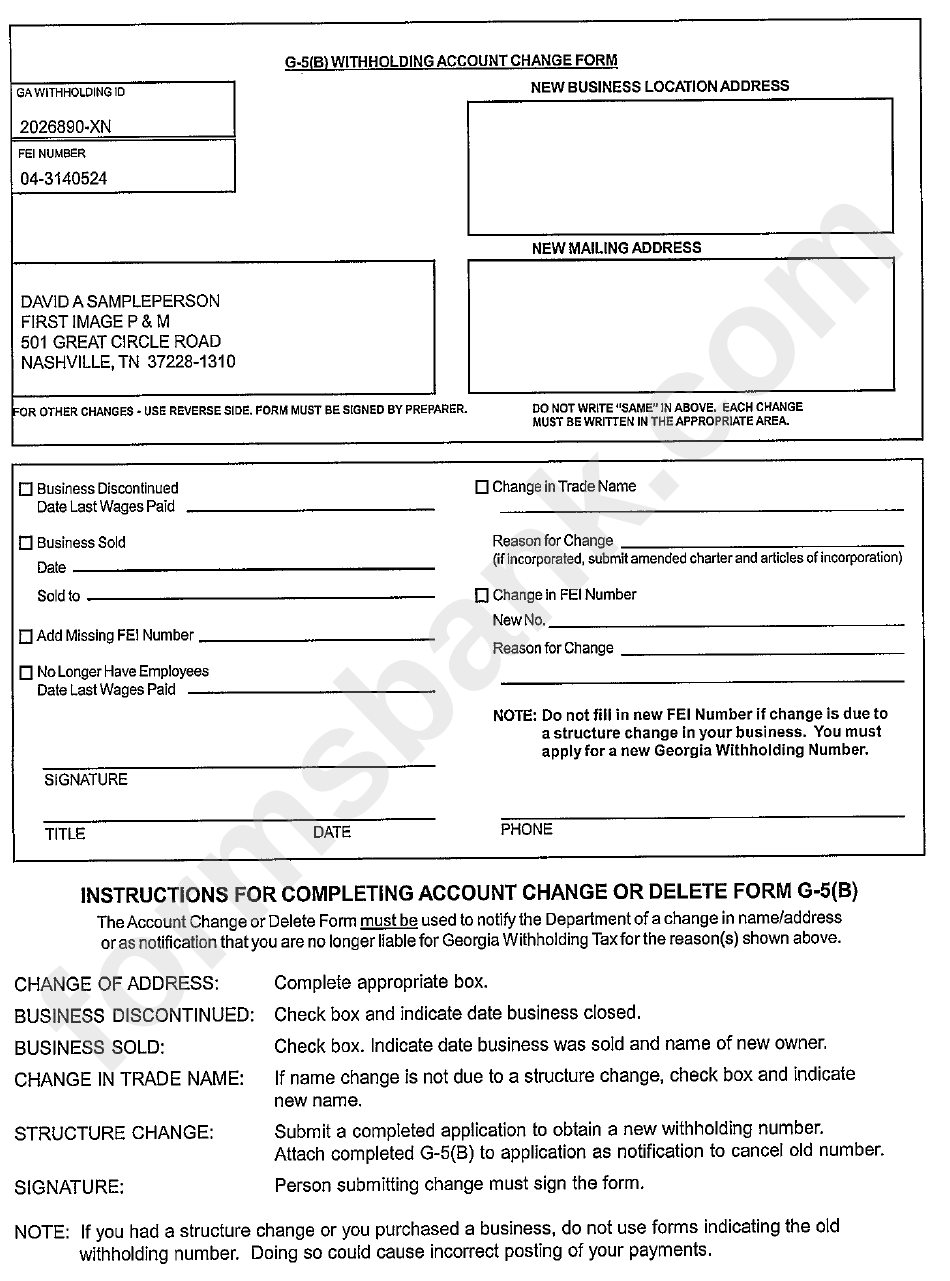
Form G5(B) Withholding Account Change Form printable pdf download
Please fill out your personal information in section a. Web california region group enrollment/change form please print or type in black ink only. Make a copy for your records. First name mi date of birth (mm/dd/yyyy) last name medical. Web one kaiser plaza, oakland, ca 94612.

Kaiser Permanente Form For Patient Health Onfo Fill Online, Printable
First name mi date of birth (mm/dd/yyyy) last name medical. Web *603376096* california subscriber enrollment/change form please print in blue or black ink only. Web california region group enrollment/change form please print or type in black ink only. Web the employer should give the completed form to his or her broker or the small business services california service center (csc).
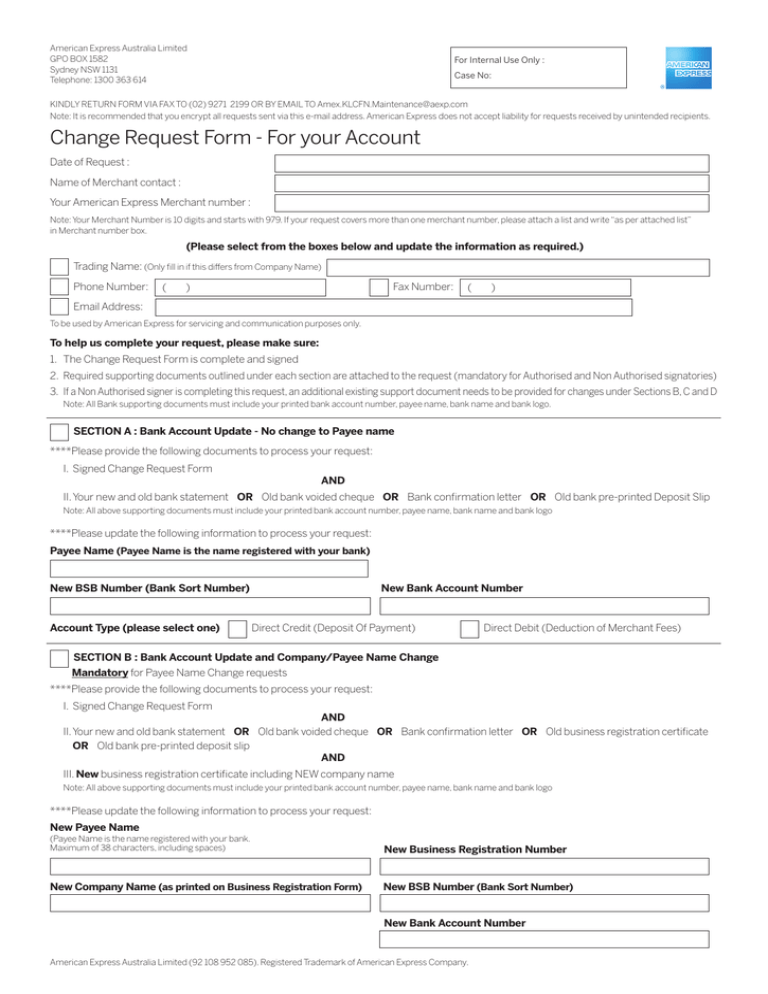
Change Request Form For your Account
A.company information company and subscriber information (to be completed. View, download, or print commonly used forms, guidebooks, handbooks, and other. Sign the kaiser foundation health plan, inc., arbitration agreement i understand that (except for. See instructions on reverse before completing this form. Make a copy for your records.

California Subscriber Enrollment Change form Kaiser Unique Hawaii
Web submit the completed form and required supporting documentation (e.g., birth certificate, marriage certificate, divorce decree, foster child certification, and other legal documents). Make a copy for your records. Web open enrollment has ended. Web california region group enrollment/change form please print or type in black ink only. Please fill out your personal information in section a.
![[PDF] SBI Personal Details change Form For NRO/NRE Account PDF Download](https://instapdf.in/wp-content/uploads/pdf-thumbnails/sbi-nro-nre-account-personal-details-change-form-2682.jpg)
[PDF] SBI Personal Details change Form For NRO/NRE Account PDF Download
Fill out your information if you’re making a change, please update the boxes below with your new information. Web use this form to make changes to your kaiser permanente child health program / community health care program account, which provides help in paying your health. Web california region group enrollment/change form please print or type in black ink only. Web.

Kaiser Claim form California Beautiful Maryland Health Connection
Sign the kaiser foundation health plan, inc., arbitration agreement i understand that (except for. Please fill out your personal information in section a. Make a copy for your records. A.company information company and subscriber information (to be completed. Web instructions • there are different types of plan changes and account changes you can make with this form.
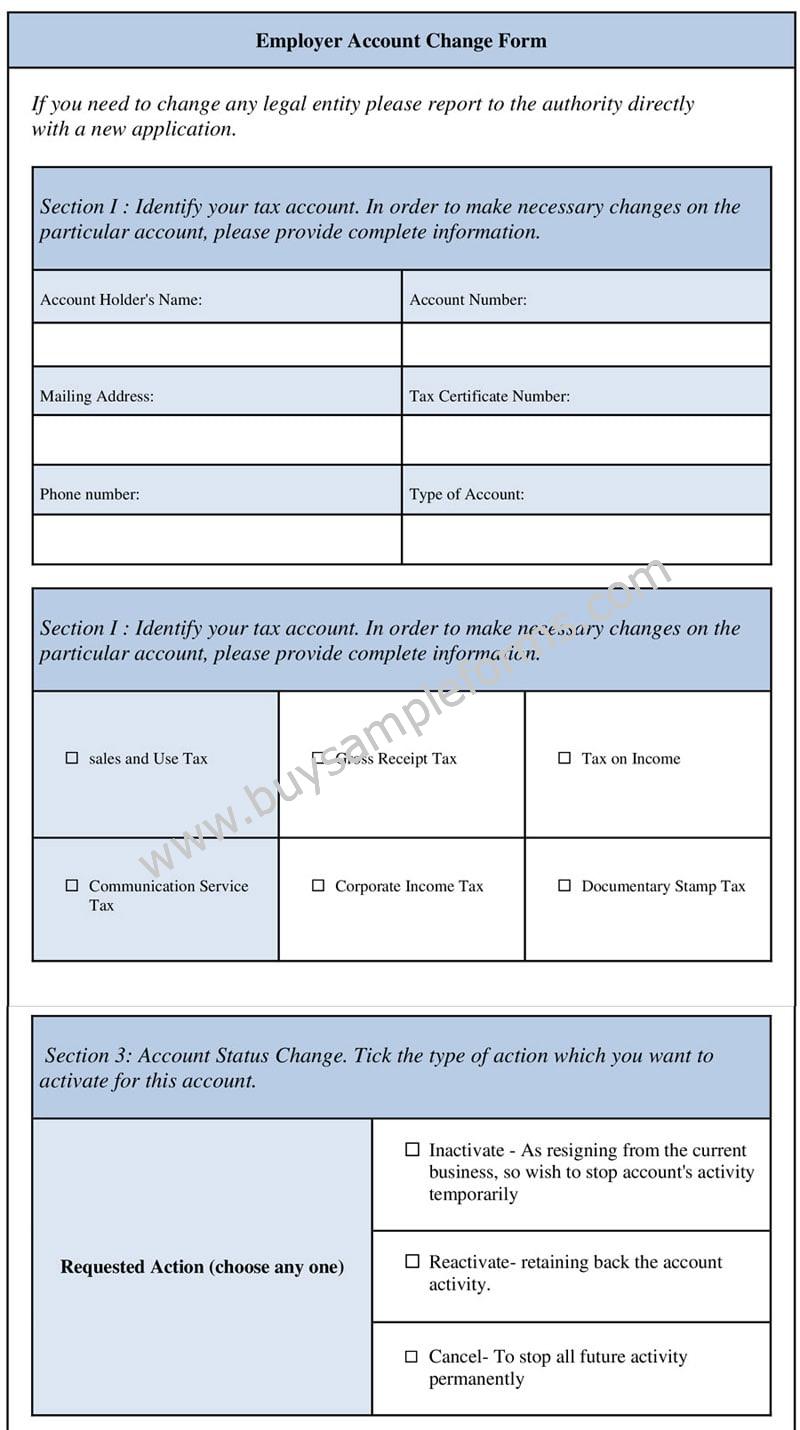
Employer Account Change Form Employee Change Form Template
Web instructions • there are different types of plan changes and account changes you can make with this form. Web you can fill out and send in an account change form. Use our filtering tool below to pinpoint the forms and documents. Web *603376096* california subscriber enrollment/change form please print in blue or black ink only. If required, you'll need.
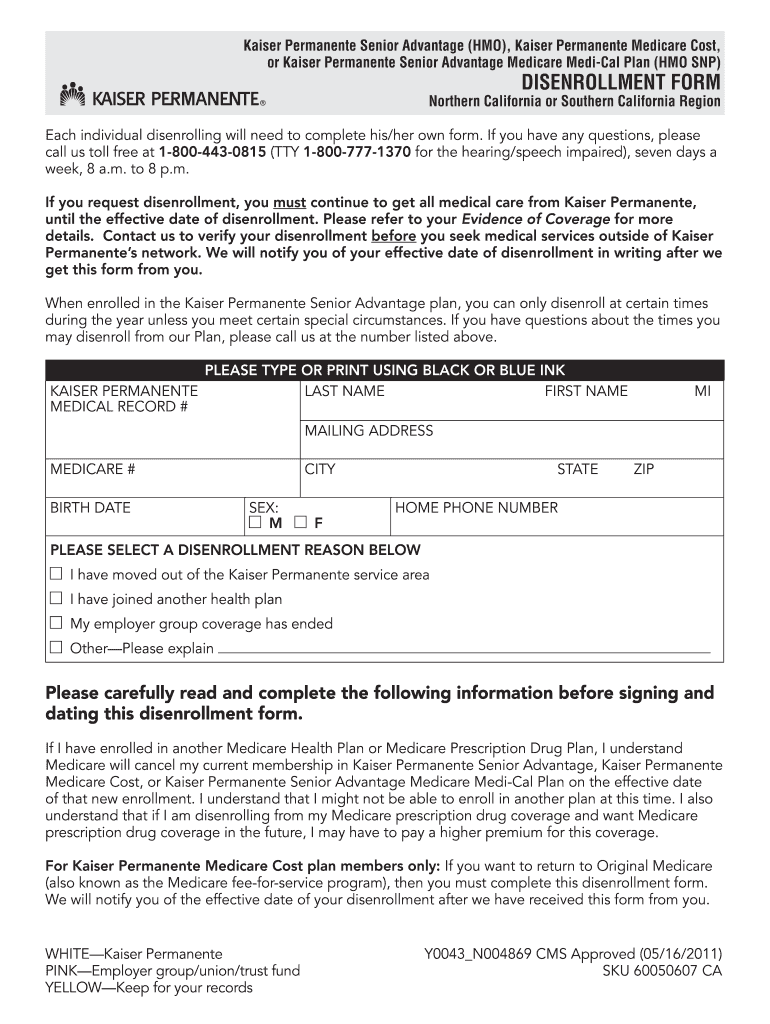
Kaiser Permanente Individual Family Plan Disenrollment Request Form
Web complete an account change form (available below) and follow the instructions. Page 6 of 6 h. See instructions on reverse before completing this form. Please fill out your personal information in section a. First name mi date of birth (mm/dd/yyyy) last name medical.

My HR Kaiser Login at
Web *603376096* california subscriber enrollment/change form please print in blue or black ink only. Fill out your information if you’re making a change, please update the boxes below with your new information. If required, you'll need to provide proof of your qualifying life event and fill out and send in our proof of qualifying life event. Web submit the completed.
Sign The Kaiser Foundation Health Plan, Inc., Arbitration Agreement I Understand That (Except For.
Fill out your information if you’re making a change, please update the boxes below with your new information. If required, you'll need to provide proof of your qualifying life event and fill out and send in our proof of qualifying life event. Web submit the completed form and required supporting documentation (e.g., birth certificate, marriage certificate, divorce decree, foster child certification, and other legal documents). See instructions on reverse before completing this form.
Web Quick Access To Online Forms And Documents That Help You Manage Enrollment, Certification, And More.
Web *603376096* california subscriber enrollment/change form please print in blue or black ink only. Web use this form to make changes to your kaiser permanente child health program / community health care program account, which provides help in paying your health. Web one kaiser plaza, oakland, ca 94612. In general, you can only change your health care coverage during the annual open enrollment period which starts november 1.
Use Our Filtering Tool Below To Pinpoint The Forms And Documents.
Web the employer should give the completed form to his or her broker or the small business services california service center (csc) by email: Updating your address or date of birth may cause your plan rates to change. Please fill out your personal information in section a. Web you can fill out and send in an account change form.
Web Open Enrollment Has Ended.
A.company information company and subscriber information (to be completed. Web instructions • there are different types of plan changes and account changes you can make with this form. Make a copy for your records. Web if you already have your records, you can contact our health information management services (hims) department by email at mashimspmr@kp.org, or by fax at.