Medicaid Hysterectomy Consent Form
Medicaid Hysterectomy Consent Form - 1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4] apple health client id. Web ohio department of medicaid. Web payment by louisiana’s medicaid program cannot be authorized for any hysterectomy performed solely for the purpose of rendering an individual permanently incapable of. Forms have retained their original form. • enter the name of the representative if the. This form is not available for ordering. Web here, you will find a library of the forms most frequently used by health care professionals. Web this form allows an individual to provide consent for sterilization. Client’s name can be typed or. Web • enter the recipient’s 13 digit medicaid number.
This form is not available for ordering. Forms have retained their original form. Specific medicaid requirements must be met and. This form is not available for ordering. Web abortion consent *see below. Web • enter the recipient’s 13 digit medicaid number. Web this form allows an individual to provide consent for sterilization. • enter the diagnosis code. Web payment by louisiana’s medicaid program cannot be authorized for any hysterectomy performed solely for the purpose of rendering an individual permanently incapable of. Web forms are sorted by those that are strictly for internal purposes and communication and those that are sent outside of the agency.
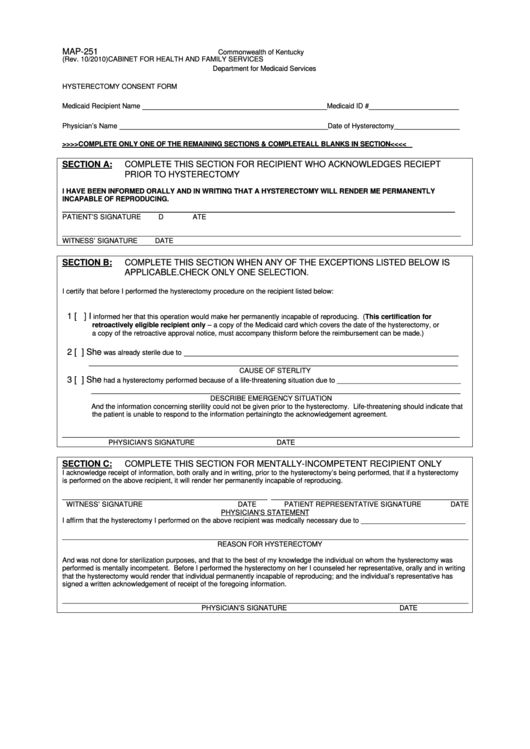
Web forms are sorted by those that are strictly for internal purposes and communication and those that are sent outside of the agency. Client’s name can be typed or. Web a copy of the mco id card, which covers the date of the hysterectomy, or a copy of the retroactive approval notice, must accompany this form before reimbursement can be. Looking for a form but don’t see it here? The hysterectomy was performed in a life threatening emergency in which prior acknowledgement was not possible. Please contact your provider representative for. Forms have retained their original form. Web ohio department of medicaid. Describe the nature of the emergency: Abortion consent, spanish *see below.

Ohio Medicaid Hysterectomy Consent Form 2022 Printable Consent Form 2022
Web • enter the recipient’s 13 digit medicaid number. Web to submit a sterilization consent form. • enter the diagnosis code. Client’s name can be typed or. Web 18 rows online form for certain hospital providers to electronically request.
Form Map251 Hysterectomy Consent Form printable pdf download
This form is not available for ordering. Client’s name can be typed or. Web • enter the recipient’s 13 digit medicaid number. Web 18 rows online form for certain hospital providers to electronically request. This form is not available for ordering.
PPT DEPARTMENT OF PUBLIC HEALTH AND HUMAN SERVICES HEALTH RESOURCES
This form is not available for ordering. Web provider references forms the following forms, for use in the indiana health coverage programs (ihcp), are maintained by the indiana family and social services. Web here, you will find a library of the forms most frequently used by health care professionals. Describe the nature of the emergency: Client’s name can be typed.

Hysterectomy Consent Form For Ohio Medicaid 2023 Printable Consent
Web ☐ abortion consent form ☐ hysterectomy consent form ☐ medical records ☐ corrected claim ☐ invoice ☐ other health insurance information ☐ er level of payment. This form is not available for ordering. Web a copy of the mco id card, which covers the date of the hysterectomy, or a copy of the retroactive approval notice, must accompany this.

Hysterectomy Consent Form
Web a copy of the mco id card, which covers the date of the hysterectomy, or a copy of the retroactive approval notice, must accompany this form before reimbursement can be. Web forms are sorted by those that are strictly for internal purposes and communication and those that are sent outside of the agency. Insert the patient’s medicaid identification. Web.

Updated Hysterectomy Consent Form Washington State Local Health
This form is not available for ordering. Web here, you will find a library of the forms most frequently used by health care professionals. Web nc medicaid reproductive health forms including abortion, hysterectomy, pregnancy medical home, pregnancy risk screening and sterilization. Looking for a form but don’t see it here? Web a copy of the mco id card, which covers.

Consent Form Blood Transfusion 2023
Web provider references forms the following forms, for use in the indiana health coverage programs (ihcp), are maintained by the indiana family and social services. Please contact your provider representative for. 1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4] apple health client id. Specific medicaid requirements must be met and..

Ohio Medicaid Hysterectomy Consent Form 2023
Describe the nature of the emergency: Statements are also included for an interpreter, a person obtaining consent, and a physician. Looking for a form but don’t see it here? Web • enter the recipient’s 13 digit medicaid number. Health benefits/nc medicaid (dhb) form effective date.

Louisiana Form 96 A Fill Online, Printable, Fillable, Blank pdfFiller
This form is not available for ordering. Web here, you will find a library of the forms most frequently used by health care professionals. 1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4] apple health client id. Web instructions for completing the hysterectomy acknowledgment form always complete this section client name:.

Qld housing assistance application form 7 fillable pdf Australian
Describe the nature of the emergency: Web forms are sorted by those that are strictly for internal purposes and communication and those that are sent outside of the agency. Web here, you will find a library of the forms most frequently used by health care professionals. Web nc medicaid reproductive health forms including abortion, hysterectomy, pregnancy medical home, pregnancy risk.
Web 18 Rows Online Form For Certain Hospital Providers To Electronically Request.
Please contact your provider representative for. Describe the nature of the emergency: Web to submit a sterilization consent form. Web payment by louisiana’s medicaid program cannot be authorized for any hysterectomy performed solely for the purpose of rendering an individual permanently incapable of.
Complete Section I And Either Section Ii Or Section Iii.
Forms have retained their original form. Web provider references forms the following forms, for use in the indiana health coverage programs (ihcp), are maintained by the indiana family and social services. This form is not available for ordering. • enter the name of the representative if the.
Web A Copy Of The Mco Id Card, Which Covers The Date Of The Hysterectomy, Or A Copy Of The Retroactive Approval Notice, Must Accompany This Form Before Reimbursement Can Be.
This form is not available for ordering. Statements are also included for an interpreter, a person obtaining consent, and a physician. Web • enter the recipient’s 13 digit medicaid number. • enter the diagnosis code.
Web Abortion Consent *See Below.
1 patient information [19] [9] patient name (print first and last name) patient date of birth (mm/dd/yyyy) [25][4] apple health client id. Web instructions for completing the hysterectomy acknowledgment form always complete this section client name: Specific medicaid requirements must be met and. Web ☐ abortion consent form ☐ hysterectomy consent form ☐ medical records ☐ corrected claim ☐ invoice ☐ other health insurance information ☐ er level of payment.