Medical Release For Dental Treatment Form
Medical Release For Dental Treatment Form - Web your state dental society may also be able to provide information about state law requirements. I understand that i may withdraw or revoke my permission at any time. With a free online dental treatment waiver form, you can. Web dental records release form. Please complete this form entirely so. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Your professional liability insurance company may consider such a. Most recent ____ years of record my dental records for the following date(s): Contact information for the patient’s primary health care. Ensure that the form is suitable for your scenario and.
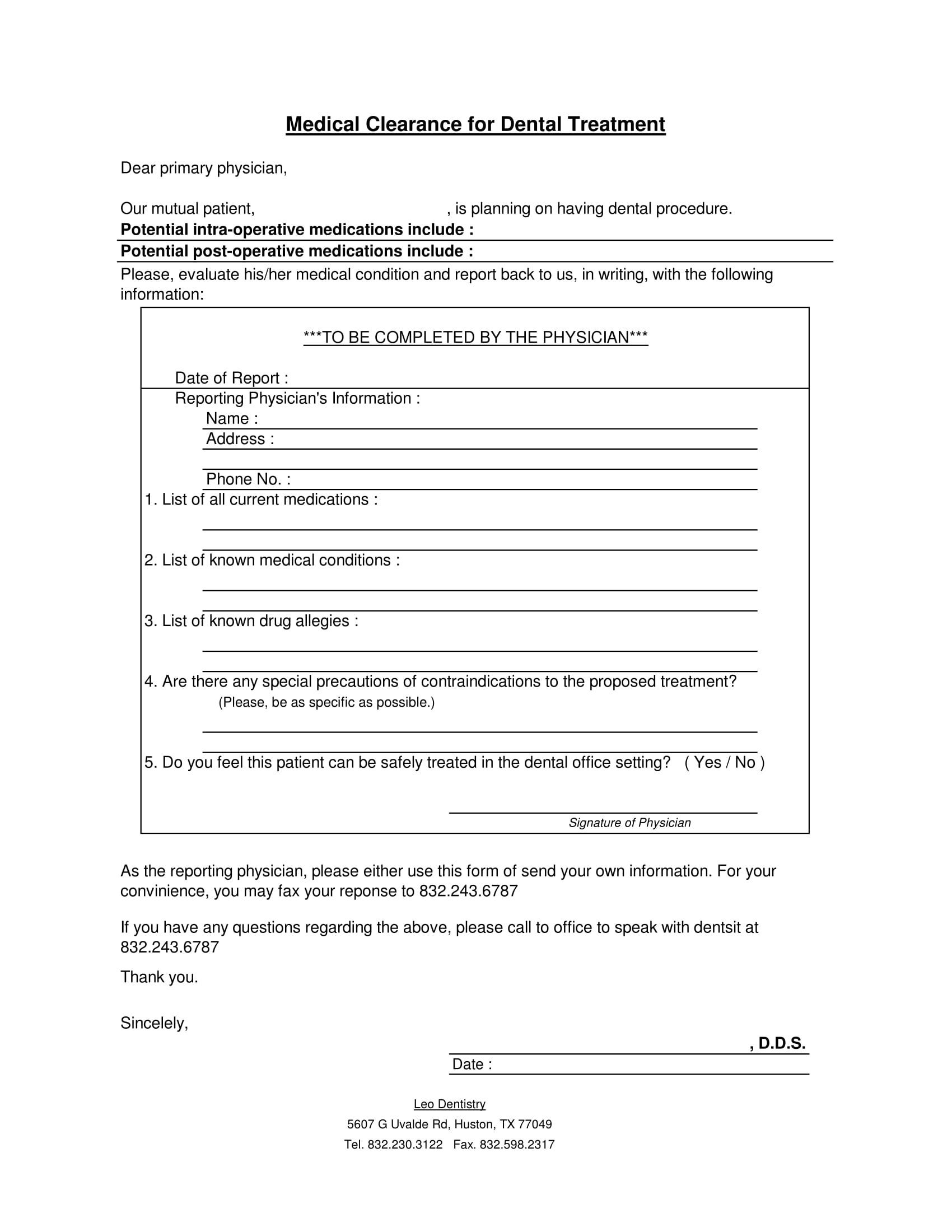
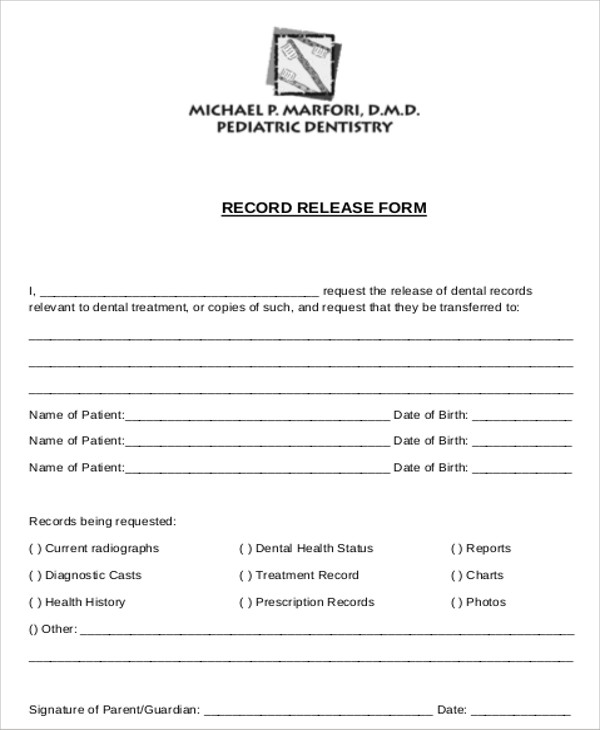
The patient’s health conditions and illnesses. Web the dental medical release form template is a fairly universal form, and takes minimal editing to get you started. Web we appreciate your assistance in providing optimum care for our patient. A simple release form for release of the record to either the patient or another health care provider may be signed by the patient and become a part of the. Simply add the details that are specific to your own. Qtl dental 121 n 31st street suite a temple, tx 76504 phone #: Web medical clearance for dental treatment allison & associates 15 aviemore drive pinehurst, nc 28374 www.pinehurstdentist.com. With a free online dental treatment waiver form, you can. Web your state dental society may also be able to provide information about state law requirements. _____, certify that i am the parent or legal guardian of the minor listed below, and as such, i hereby convey.
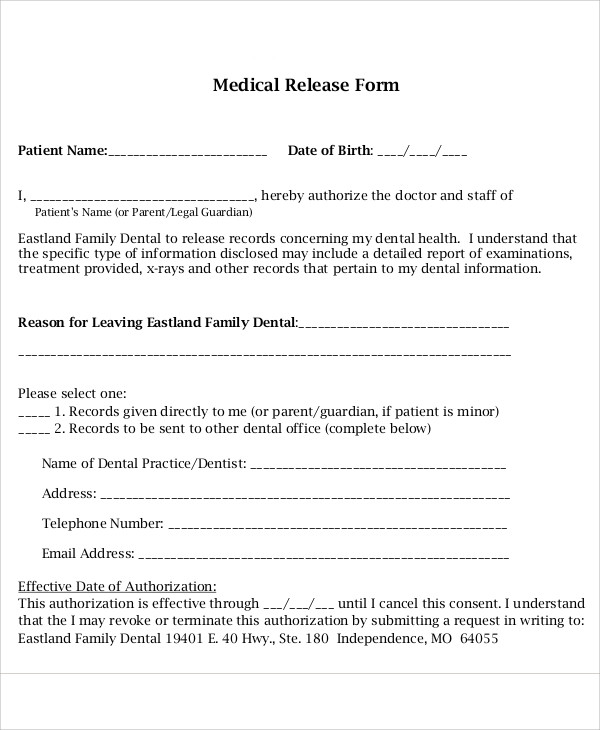
Web medical clearance for dental treatment allison & associates 15 aviemore drive pinehurst, nc 28374 www.pinehurstdentist.com. Web the dental medical release form template is a fairly universal form, and takes minimal editing to get you started. With a free online dental treatment waiver form, you can. Please complete this form entirely so. Web my dental information relating to the following treatment or condition: Use this free authorization to release dental information. Please sign and fax form to: Web some of the issues that can be covered in a health history form include: Web a dental information authorization form allows patients to authorize the release of their dental records to a third party. _____, certify that i am the parent or legal guardian of the minor listed below, and as such, i hereby convey.
FREE 22+ Sample Medical Release Forms in PDF Word Excel
Simply add the details that are specific to your own. Web a dental treatment waiver is a document used by medical practices to obtain patient consent before treating them. Most recent ____ years of record my dental records for the following date(s): Web dental records release form. Web medical clearance for dental treatment patient’s name:_____ d.o.b:_____ date of last physical.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Web your state dental society may also be able to provide information about state law requirements. Please complete this form entirely so. Qtl dental 121 n 31st street suite a temple, tx 76504 phone #: Use this free authorization to release dental information. Web if you want to know how to get the medical release for dental treatment in a.
FREE 44+ Medical Forms in PDF
With a free online dental treatment waiver form, you can. Qtl dental 121 n 31st street suite a temple, tx 76504 phone #: Most recent ____ years of record my dental records for the following date(s): _____, certify that i am the parent or legal guardian of the minor listed below, and as such, i hereby convey. Please sign and.
FREE 11+ Sample Dental Release Forms in MS Word PDF
I understand that i may withdraw or revoke my permission at any time. A simple release form for release of the record to either the patient or another health care provider may be signed by the patient and become a part of the. Web a dental treatment waiver is a document used by medical practices to obtain patient consent before.
Generic Medical Release Form Template Business
Your professional liability insurance company may consider such a. Web some of the issues that can be covered in a health history form include: With a free online dental treatment waiver form, you can. I understand that i may withdraw or revoke my permission at any time. Web medical clearance for dental treatment patient’s name:_____ d.o.b:_____ date of last physical.

Free Medical Release Form Template Continuum
The dental records release form is a document given by a dental. Web we appreciate your assistance in providing optimum care for our patient. Web my dental information relating to the following treatment or condition: Simply add the details that are specific to your own. Ensure that the form is suitable for your scenario and.
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Qtl dental 121 n 31st street suite a temple, tx 76504 phone #: The patient’s health conditions and illnesses. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Contact information for the patient’s primary health care. Web the dental medical release form.
FREE 11+ Sample Dental Release Forms in MS Word PDF
Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Web the dental medical release form template is a fairly universal form, and takes minimal editing to get you started. Contact information for the patient’s primary health care. Please complete this form entirely.
FREE 8+ Sample Dental Records Release Forms in MS Word PDF
Contact information for the patient’s primary health care. Web if you want to know how to get the medical release for dental treatment in a matter of clicks, follow the guide below: Simply add the details that are specific to your own. Your professional liability insurance company may consider such a. Web my dental information relating to the following treatment.
FREE 11+ Sample Dental Release Forms in MS Word PDF
Web if you want to know how to get the medical release for dental treatment in a matter of clicks, follow the guide below: With a free online dental treatment waiver form, you can. ___ this patient is optimized for surgery and. Ensure that the form is suitable for your scenario and. The dental records release form is a document.
The Patient’s Health Conditions And Illnesses.
Web a dental information authorization form allows patients to authorize the release of their dental records to a third party. Web medical clearance for dental treatment allison & associates 15 aviemore drive pinehurst, nc 28374 www.pinehurstdentist.com. Your professional liability insurance company may consider such a. Web a dental treatment waiver is a document used by medical practices to obtain patient consent before treating them.
Web We Appreciate Your Assistance In Providing Optimum Care For Our Patient.
I understand that i may withdraw or revoke my permission at any time. Please sign and fax form to: A simple release form for release of the record to either the patient or another health care provider may be signed by the patient and become a part of the. Web teeth, fractured teeth or fillings, loose teeth or other oral pathology and no anticipation of dental care within the next 6 months.
Web Some Of The Issues That Can Be Covered In A Health History Form Include:
Use this free authorization to release dental information. Web medical clearance for dental treatment patient’s name:_____ d.o.b:_____ date of last physical exam:_____ dear physician: With a free online dental treatment waiver form, you can. Please complete this form entirely so.
___ This Patient Is Optimized For Surgery And.
_____, certify that i am the parent or legal guardian of the minor listed below, and as such, i hereby convey. Simply add the details that are specific to your own. Web my dental information relating to the following treatment or condition: Web all treatment information information specifically related to these treatment dates starting date: