Metroplus Authorization Request Form
Metroplus Authorization Request Form - Web metroplus prior authorization forms | covermymeds metroplus's preferred method for prior authorization requests our electronic prior authorization (epa) solution provides a safety net to ensure the right information needed for a determination gets to patients' health plans as fast as possible. Web complete metroplus authorization form online with us legal forms. Basic plan is free for nyc workers and their families! 1.866.255.7569 information on this form is protected health information and subject to all privacy and security regulations under hipaa. 1.800.475.6387 pharmacy benefit manager fax no: Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to the service type). Start a request scroll to learn more why covermymeds Please do not use this form for outpatient therapy or home care. Web metroplushealth actively maintains a library of resources and forms to assist our participating providers treat their patients. Easily fill out pdf blank, edit, and sign them.
Start a request scroll to learn more why covermymeds Metroplus health plan plan phone no. Web authorization grid (coming soon, 2023 updates in progress) provider orientation and attestation: Prior authorization & exceptions forms aba universal request form Metroplus health plan plan phone no: Save or instantly send your ready documents. Explore our resources for providers. (if applicable) new request for services request for additional services request to extend date(s) on a current authorization period Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to the service type). Web metroplus prior authorization forms | covermymeds metroplus's preferred method for prior authorization requests our electronic prior authorization (epa) solution provides a safety net to ensure the right information needed for a determination gets to patients' health plans as fast as possible.
Easily fill out pdf blank, edit, and sign them. Explore our resources for providers. Basic plan is free for nyc workers and their families! Save or instantly send your ready documents. Web metroplus prior authorization forms | covermymeds metroplus's preferred method for prior authorization requests our electronic prior authorization (epa) solution provides a safety net to ensure the right information needed for a determination gets to patients' health plans as fast as possible. Please go to the form download link to retrieve the appropriate forms for these services. Web want to become a metroplushealth provider? Start a request scroll to learn more why covermymeds Web complete metroplus authorization form online with us legal forms. Please do not use this form for outpatient therapy or home care.
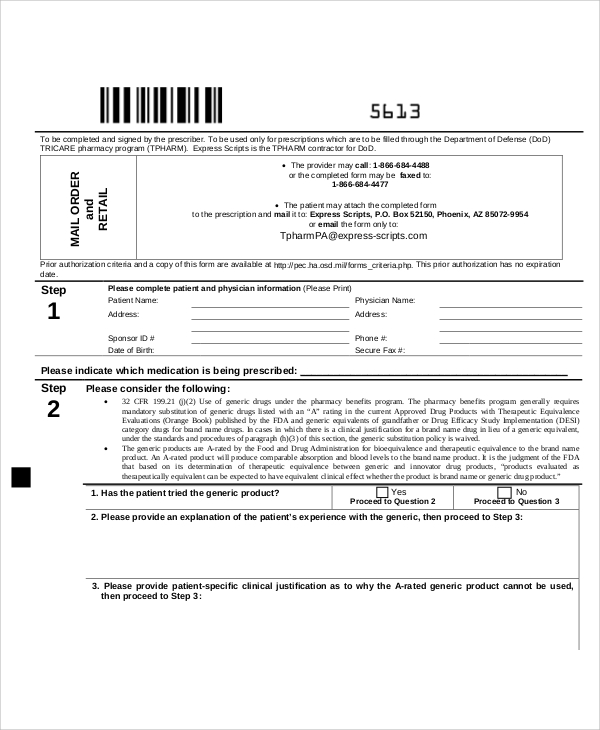
Medication Prior Authorization Request Form printable pdf download
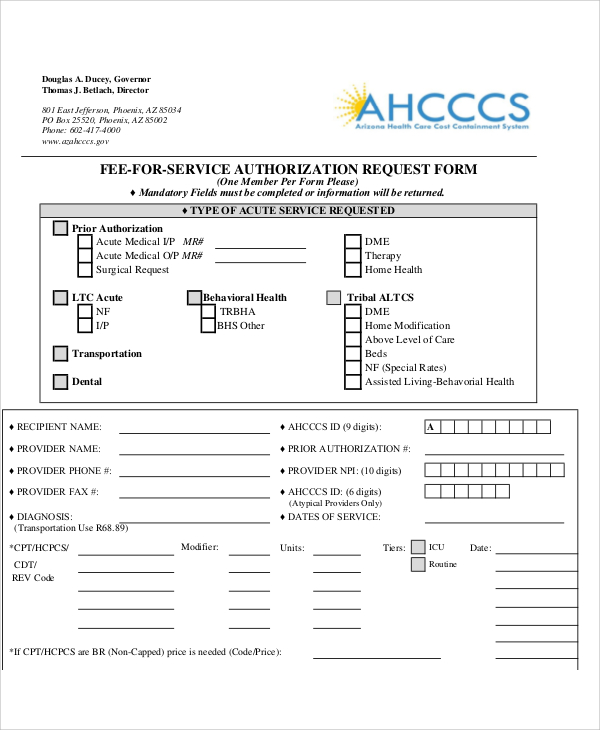
Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to the service type). Prior authorization & exceptions forms aba universal request form Metroplus health plan plan phone no. 1.800.475.6387 pharmacy benefit manager fax no: Please go to the form download link to retrieve the appropriate forms for.

Metroplus Authorization Request Form
Please do not use this form for outpatient therapy or home care. Web authorization grid (coming soon, 2023 updates in progress) provider orientation and attestation: Web want to become a metroplushealth provider? Web metroplushealth actively maintains a library of resources and forms to assist our participating providers treat their patients. Web complete metroplus authorization form online with us legal forms.
Fillable Prior Authorization Request Form printable pdf download
Save or instantly send your ready documents. (if applicable) new request for services request for additional services request to extend date(s) on a current authorization period 1.800.475.6387 pharmacy benefit manager fax no: Web nys medicaid prior authorization request form for prescriptions plan name: 1.866.255.7569 information on this form is protected health information and subject to all privacy and security regulations.
FREE 10+ Sample Authorization Request Forms in MS Word PDF
Start a request scroll to learn more why covermymeds Web nys medicaid prior authorization request form for prescriptions plan name: Web metroplushealth actively maintains a library of resources and forms to assist our participating providers treat their patients. Web authorization grid (coming soon, 2023 updates in progress) provider orientation and attestation: Basic plan is free for nyc workers and their.
FREE 10+ Sample Authorization Request Forms in MS Word PDF
Web want to become a metroplushealth provider? Please do not use this form for outpatient therapy or home care. Metroplus health plan plan phone no. 1.800.475.6387 pharmacy benefit manager fax no: Core provider service initiation notification form:

Work Authorization Request Form Sample Templates Sample Templates
Web want to become a metroplushealth provider? Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to the service type). Start a request scroll to learn more why covermymeds Core provider service initiation notification form: Please do not use this form for outpatient therapy or home care.

Metroplus Authorization Request Form
Save or instantly send your ready documents. Please do not use this form for outpatient therapy or home care. Web want to become a metroplushealth provider? Prior authorization & exceptions forms aba universal request form Web complete metroplus authorization form online with us legal forms.
FREE 10+ Sample Authorization Request Forms in MS Word PDF
Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to the service type). Core provider service initiation notification form: Web metroplushealth actively maintains a library of resources and forms to assist our participating providers treat their patients. Easily fill out pdf blank, edit, and sign them. 1.866.255.7569.
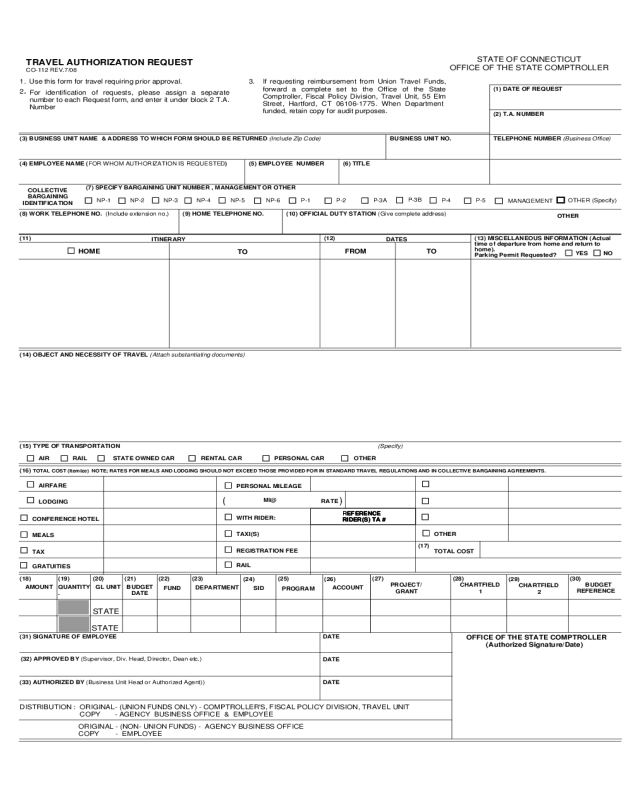
2022 Travel Authorization Form Fillable, Printable PDF & Forms Handypdf
Save or instantly send your ready documents. Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to the service type). 1.800.475.6387 pharmacy benefit manager fax no: Metroplus health plan plan phone no. Web metroplushealth actively maintains a library of resources and forms to assist our participating providers.
FREE 10+ Sample Authorization Request Forms in MS Word PDF
Prior authorization & exceptions forms aba universal request form Web metroplushealth actively maintains a library of resources and forms to assist our participating providers treat their patients. Basic plan is free for nyc workers and their families! Web nys medicaid prior authorization request form for prescriptions plan name: Please do not use this form for outpatient therapy or home care.
1.866.255.7569 Pharmacy Benefit Manager Phone No:
Metroplus health plan plan phone no. Prior authorization & exceptions forms aba universal request form Web metroplus prior authorization forms | covermymeds metroplus's preferred method for prior authorization requests our electronic prior authorization (epa) solution provides a safety net to ensure the right information needed for a determination gets to patients' health plans as fast as possible. Easily fill out pdf blank, edit, and sign them.
(If Applicable) New Request For Services Request For Additional Services Request To Extend Date(S) On A Current Authorization Period
Page 1 of 2 nys medicaid prior authorization request form for prescriptions Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to the service type). Basic plan is free for nyc workers and their families! Save or instantly send your ready documents.
1.800.475.6387 Pharmacy Benefit Manager Fax No:
Please do not use this form for outpatient therapy or home care. Explore our resources for providers. Web nys medicaid prior authorization request form for prescriptions plan name: Metroplus health plan plan phone no:
Web Authorization Grid (Coming Soon, 2023 Updates In Progress) Provider Orientation And Attestation:
Web complete metroplus authorization form online with us legal forms. Web want to become a metroplushealth provider? Start a request scroll to learn more why covermymeds Core provider service initiation notification form: