Molina Appeal Form Ohio
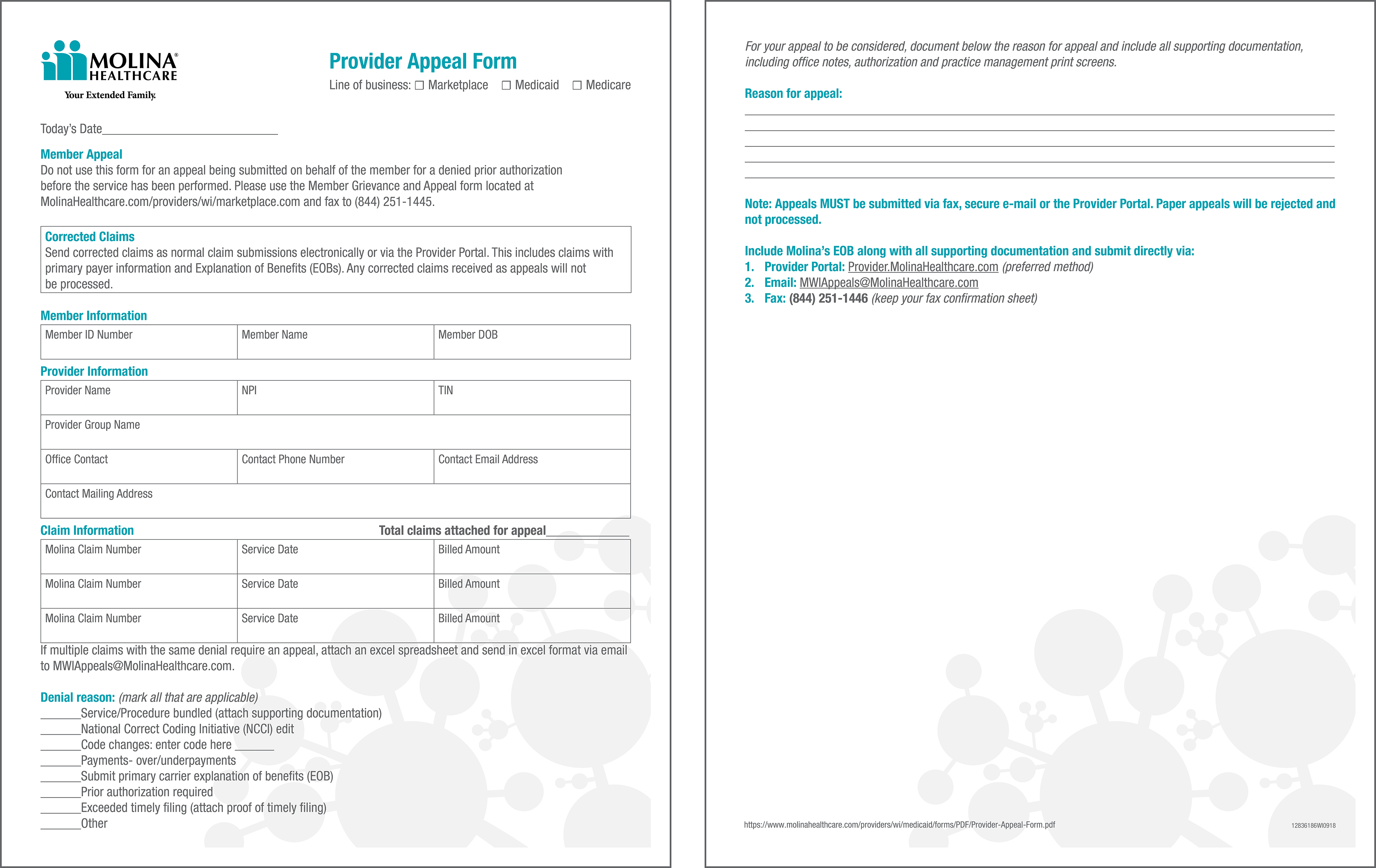
Molina Appeal Form Ohio - Please include a copy of the eob with the appeal and any supporting documentation. If you have someone else submit on. Nevada member appeals po box 401820 las vegas, nv 89140 if you need a copy of the appeal request form (coming soon) you can call member services or download and print a copy. We cannot process your appeal. Web provider claims appeal request form. Web if molina medicare or one of our plan providers refuses to give you a service you think should be covered, you can file an appeal. Web appeal representative form you must sign. Include two possible dates and times a licensed professional is available to conduct the review with a molina medical director. You may file an appeal by calling member services or by writing us and sending it by mail or by fax. Web please upload this completed form and any supporting documentation through the following methods:
If you have someone else submit on. Web prior authorization lookup tool. How to file a complaint/grievance. Web member appeal form if you do not agree with a decision made by your managed care entity (mce), you should contact the mce as soon as possible. To 5 p.m., monday to friday. Molina healthcare of ohio, inc. Fill out this form completely. Web instructions for filing a grievance/appeal: Describe the issue(s) in as much. Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina mycare ohio medicaid at:
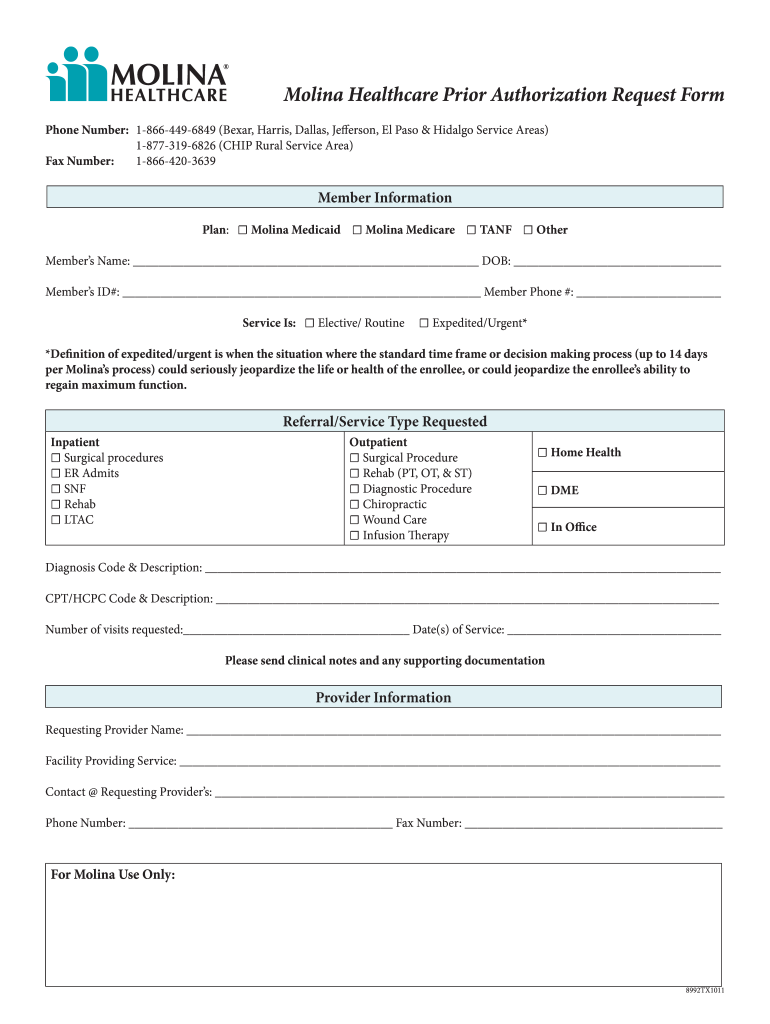
How to file a complaint/grievance. Describe the issue(s) in as much. Web send molina dispute resolution form via email, link, or fax. You can also download it, export it or print it out. This form and send it back to molina healthcare. How to appeal a denial. Web prior authorization lookup tool. Web molina healthcare provider services agreement home health care mycare ohio uniform authorization request form abortion, hysterectomy and sterilization odm consent to sterilization form guidelines for completing consent to sterilization form odm consent to hysterectomy form odm abortion certification form other forms and resources Web you may contact molina for assistance with filing your complaint over the phone, by mail or fax using the following contact information. Web instructions for filing a grievance/appeal:
Brittany Long Molina Healthcare
Type text, add images, blackout confidential details, add comments, highlights and more. 711) write a letter to: Web instructions for filing a grievance/appeal: Web an appeal can be filed when you do not agree with molina medicare’s decision to: Molina healthcare of ohio, inc.

Yadier Molina drops appeal, serves onegame suspension Wednesday MLB
711) write a letter to: Deny payment for services provided. Describe the issue(s) in as much detail as possible. You can ask for one authorization reconsideration To learn more, click on one of the links below:

Special Advertisements The Ohio Council Conference
Appoint to request an appeal on my behalf and serve as my representative throughout the appeal process. Web you may contact molina for assistance with filing your complaint over the phone, by mail or fax using the following contact information. Please include a copy of the eob with the appeal and any supporting documentation. Appeals and grievances unit p.o. Type.
Molina healthcare provider new group change form
Attach copies of any records you wish to submit. Fill out this form completely. Sign it in a few clicks. Stop, suspend, reduce or deny a service or; Molina healthcare of ohio, inc.
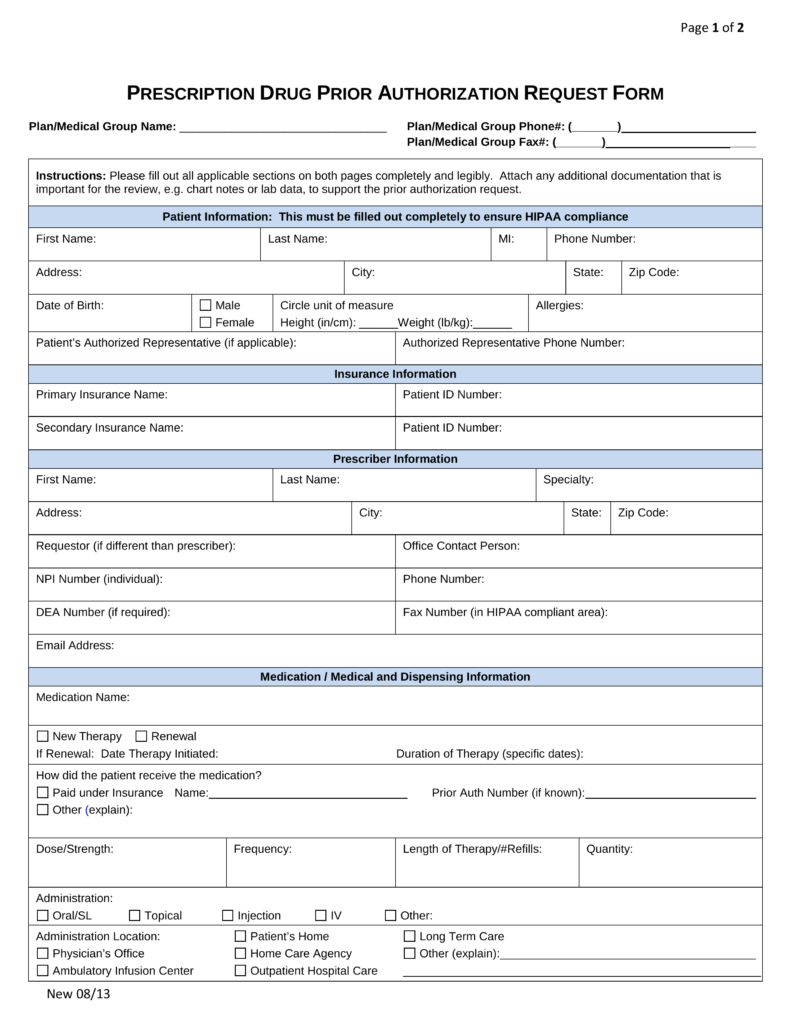
Free Medicaid (Rx) Prior Authorization Forms PDF eForms
Attach copies of any records you wish to submit. Describe the issue(s) in as much detail as possible. Web to file your appeal, you can: Web an appeal can be filed when you do not agree with molina medicare’s decision to: 711) write a letter to:

Fillable Virginia Medicaid/famis Appeal Request Form printable pdf download
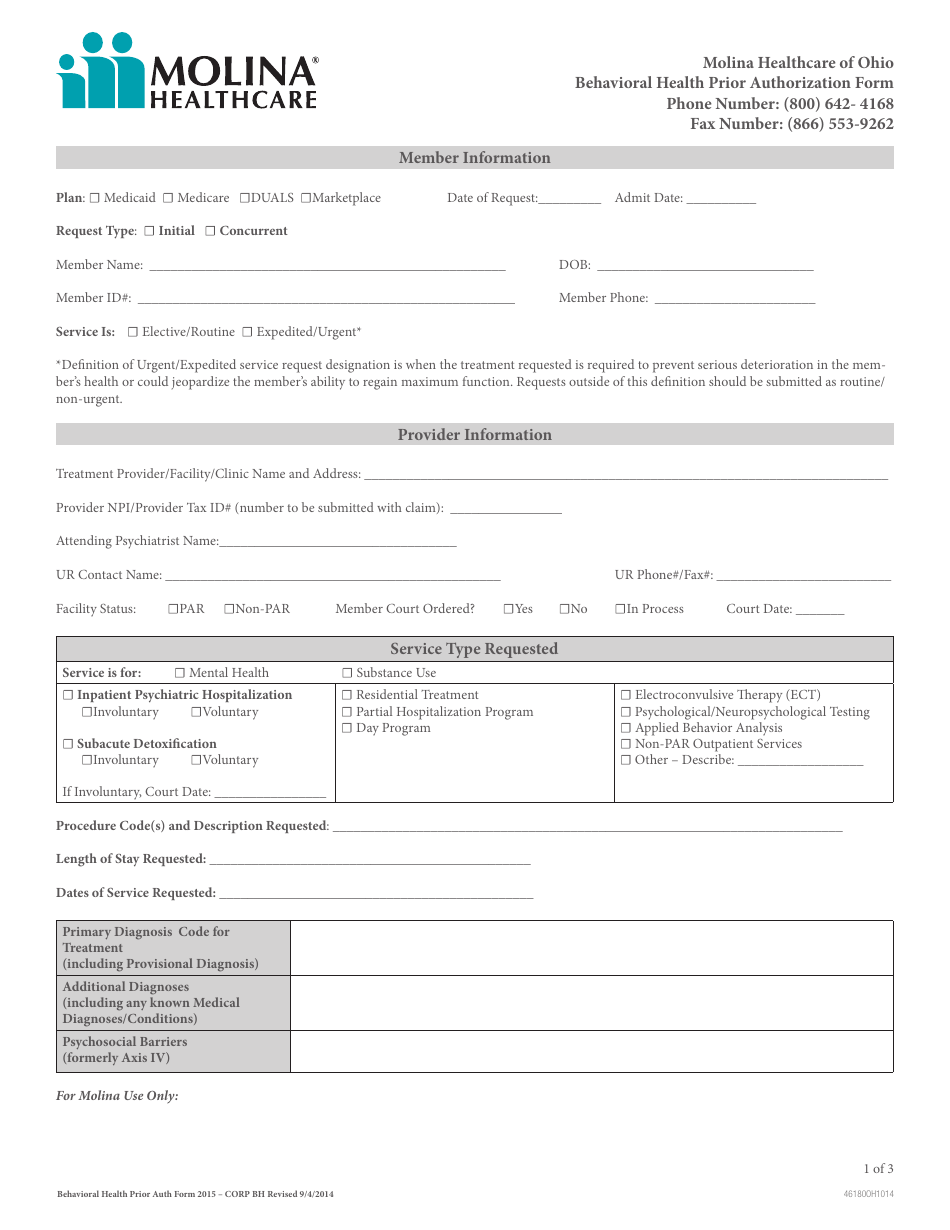
If you have someone else submit on your. Describe the issue(s) in as much. Include two possible dates and times a licensed professional is available to conduct the review with a molina medical director. Appeals and grievances unit p.o. Web if molina medicare or one of our plan providers refuses to give you a service you think should be covered,.

Molina Medicare Pa Forms Universal Network
You have 60 days from the date on the notice of action to file an appeal with molina healthcare. If molina medicare or one of our plan providers reduces or cuts back on services or benefits you have. Web the state hearing form (included with the noa) to the address or fax number listed on the form. How to file.
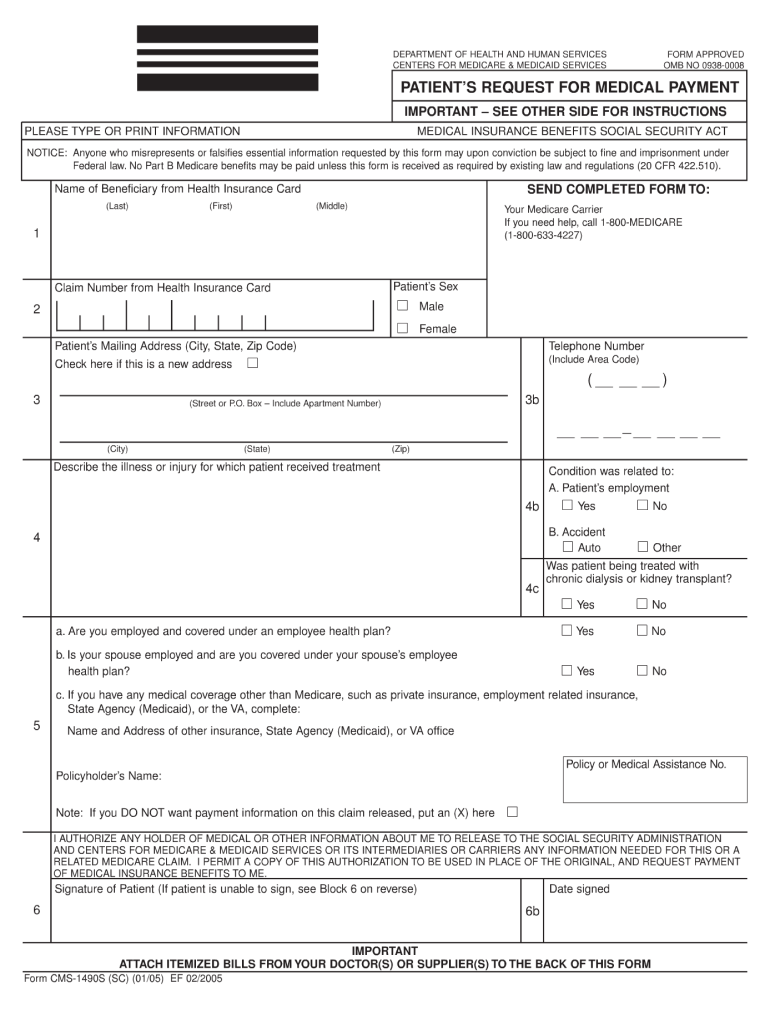
Patient's Request Fill Out and Sign Printable PDF Template signNow
Web the state hearing form (included with the noa) to the address or fax number listed on the form. Web if molina medicare or one of our plan providers refuses to give you a service you think should be covered, you can file an appeal. Web an appeal can be filed when you do not agree with molina medicare’s decision.
Molina Authorization Form Fill Online, Printable, Fillable, Blank
Describe the issue(s) in as much. Molina healthcare of ohio, inc. Web instructions for filing a grievance/appeal: Appeals and grievances unit p.o. Web to file your appeal, you can:
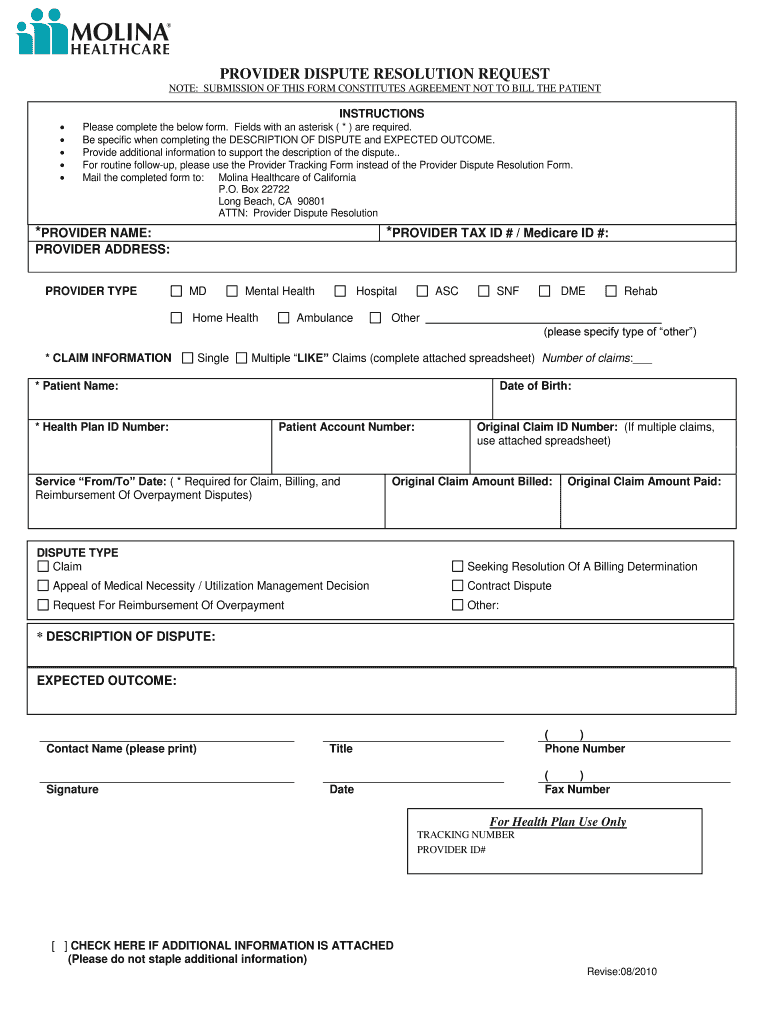
Molina provider dispute resolution form Fill out & sign online DocHub
Availity essentials portal appeal process verbally (medicaid line of business): We can help you write your appeal. Include two possible dates and times a licensed professional is available to conduct the review with a molina medical director. Web please upload this completed form and any supporting documentation through the following methods: You can ask for one authorization reconsideration
Appoint To Request An Appeal On My Behalf And Serve As My Representative Throughout The Appeal Process.
Member grievance/appeal request form instructions for filing a grievance/appeal: We can help you write your appeal. Include 2 possible dates and times a licensed professional is available to conduct the review with a molina medical director. Appeals and grievances unit p.o.
Edit Your Molina Health Care Provider Despute Cover Page Online.
You can also download it, export it or print it out. Web the state hearing form (included with the noa) to the address or fax number listed on the form. You may file an appeal by calling member services or by writing us and sending it by mail or by fax. Describe the issue(s) in as much detail as possible.
Nevada Member Appeals Po Box 401820 Las Vegas, Nv 89140 If You Need A Copy Of The Appeal Request Form (Coming Soon) You Can Call Member Services Or Download And Print A Copy.
To 5 p.m., monday to friday. Sign it in a few clicks. If you have someone else submit on. Web to file your appeal, you can:
Molina Healthcare Of Ohio, Inc.
Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina mycare ohio medicaid at: Fill out this form completely. Attach copies of any records you wish to submit. Web instructions for filing a grievance/appeal: