New Patient Medical History Form Pdf
New Patient Medical History Form Pdf - Medical history for foreign service; You can collect data about the patient and medical background with this medical history record pdf sample. How long has this pain been present? Diabetes heart problems ____________________________________ high blood pressure high cholesterol have you ever been hospital. The form is available in a digital, downloadable version or in print. If you are a current patient there is a shorter update form you ca n use. Sample medical history in pdf; Provider/person who referred you to our practice: Month / day / year (please only answer applicable questions) provider youwill be seeing:
Web whenever a new patient is admitted to the hospital for treatment, he/she is asked to fill out a medical history form along with the patient registration form. Excel | word | pdf. Web download medical history form template. Fall or other trauma date: Web object moved to here. Web new patient health history form all questions contained in this questionnaire are strictly confidential and will become part of your medical record. Years months pain history work related injury date: Medical history record pdf template is here to help you in order to know the patient's case and previous condition. Web professional medical history template. Month / day / year
No changes cancer arthritis depression/anxiety please list any additional medical conditions: A comprehensive document providing the patients’ past medical history, personal and contact details, health information, habits, living standards and family medical history with their consent to the terms and conditions. All questions contained in this questionnaire are strictly confidential and will become part of your medical record. Provider/person who referred you to our practice: This form will become part of your medical record. Web object moved to here. Web professional medical history template. But the main purpose of the form is to provide you with important information about a patient’s health history, risk factors, and care requirements. Web download or preview 6 pages of pdf version of new patient medical history form (doc: Web the patient medical history form is very important in a number of ways.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-09-scaled.jpg?w=790)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
Your answers on this form will help your health care provider get an accurate history of your medical concerns and conditions. Web new patient health history form patient name: Web gathering your patients' medical information may be a troublesome task. (please only answer applicable questions) provider youwill be seeing: Web new patient health history form thank you for taking the.
New Patient Medical History Form in Word and Pdf formats page 3 of 6
Fall or other trauma date: (please only answer applicable questions) provider youwill be seeing: Medical history for foreign service; A comprehensive document providing the patients’ past medical history, personal and contact details, health information, habits, living standards and family medical history with their consent to the terms and conditions. Excel | word | pdf.
New Patient Health History Form Template full version free software
Please fill in the circle next to your answer or clearly print your answer when asked. Medical history form in pdf; Working together, keeping you active patient information name:. Report of medical history template; For one, insurance firms use them as a basis for the insurability of a patient.
New Patient Past Medical History Form printable pdf download
Web new patient health history form. Medical history form in pdf; It is long because it is comprehensive. Web a general medical history form is a document used to record a patient’s medical history at the time of or after consultation and /or examination with a medical practitioner. Medical history for foreign service;

Patient Medical History form Template Beautiful 67 Medical History
Sample medical history in pdf; Medical history form in pdf; Web a general medical history form is a document used to record a patient’s medical history at the time of or after consultation and /or examination with a medical practitioner. (please only answer applicable questions) provider youwill be seeing: But you can collect these medical data with this medical history.
New Patient History Form printable pdf download
This form will become part of your medical record. Medical history form in pdf; Years months pain history work related injury date: Working together, keeping you active patient information name:. Web professional medical history template.
New Patient Medical History Form in Word and Pdf formats
Web the patient medical history form is very important in a number of ways. Medical history for foreign service; Diabetes heart problems ____________________________________ high blood pressure high cholesterol have you ever been hospital. Have you ever had any of the following surgeries? The physicians of one to one health originates and maintains health records describing my health history, symptoms, examination.
FREE 6+ Medical History Forms in PDF MS Word Excel
This form will become part of your medical record. A comprehensive document providing the patients’ past medical history, personal and contact details, health information, habits, living standards and family medical history with their consent to the terms and conditions. Medical history form in pdf; New patient health history form. Please fill in the circle next to your answer or clearly.
FREE 8+ Health History Forms in PDF Ms Word
A comprehensive document providing the patients’ past medical history, personal and contact details, health information, habits, living standards and family medical history with their consent to the terms and conditions. Last name first middle name you wish to be called:_______________________________________________________. This form will become part of your medical record. Web new patient intake form name: Web a general medical history.
FREE 12+ Sample Medical History Forms in PDF MS Word Excel
But you can collect these medical data with this medical history form template and you can record these data easily as a pdf with this medical history pdf template that was created by us by using jotform's new pdf editor. No changes cancer arthritis depression/anxiety please list any additional medical conditions: Sample medical history in pdf; Web new patient intake.
Web Whenever A New Patient Is Admitted To The Hospital For Treatment, He/She Is Asked To Fill Out A Medical History Form Along With The Patient Registration Form.
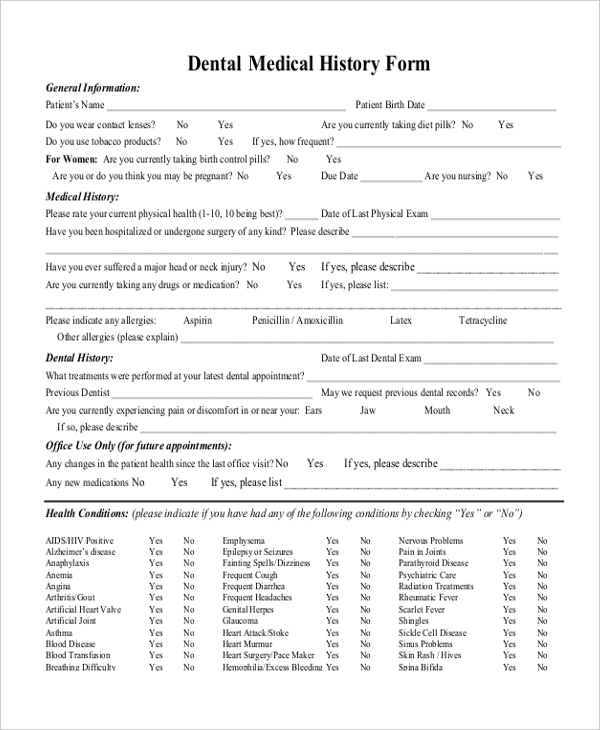
Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. It is long because it is comprehensive. Medical history record pdf template is here to help you in order to know the patient's case and previous condition. Last name first middle name you wish to be called:_______________________________________________________.
All Questions Contained In This Questionnaire Are Strictly Confidential And Will Become Part Of Your Medical Record.
Provider/person who referred you to our practice: Web gathering your patients' medical information may be a troublesome task. Have you ever been treated for any of the following medical conditions? The form is available in a digital, downloadable version or in print.
Web New Patient Health History Form.
Medical history for foreign service; Medical history form in pdf; Web the patient medical history form is very important in a number of ways. A comprehensive document providing the patients’ past medical history, personal and contact details, health information, habits, living standards and family medical history with their consent to the terms and conditions.
Working Together, Keeping You Active Patient Information Name:.
Please fill in the circle next to your answer or clearly print your answer when asked. No changes cancer arthritis depression/anxiety please list any additional medical conditions: Fall or other trauma date: Your answers on this form will help your health care provider get an accurate history of your medical concerns and conditions.