Uhc Reconsideration Form
Uhc Reconsideration Form - All forms are printable and downloadable. You have 1 year from the date of occurrence to file an appeal with the nhp. Web fill online, printable, fillable, blank uhc claim reconsideration request form. Web if you are unable to use the online reconsideration and appeals process outlined in chapter 10: Web step 1 is to file a claim reconsideration request. Single claim reconsideration/corrected claim request form this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact information and resources. Use fill to complete blank online others pdf forms for free. Web care provider administrative guides and manuals. Send filled & signed united healthcare reconsideration form 2022 or save.
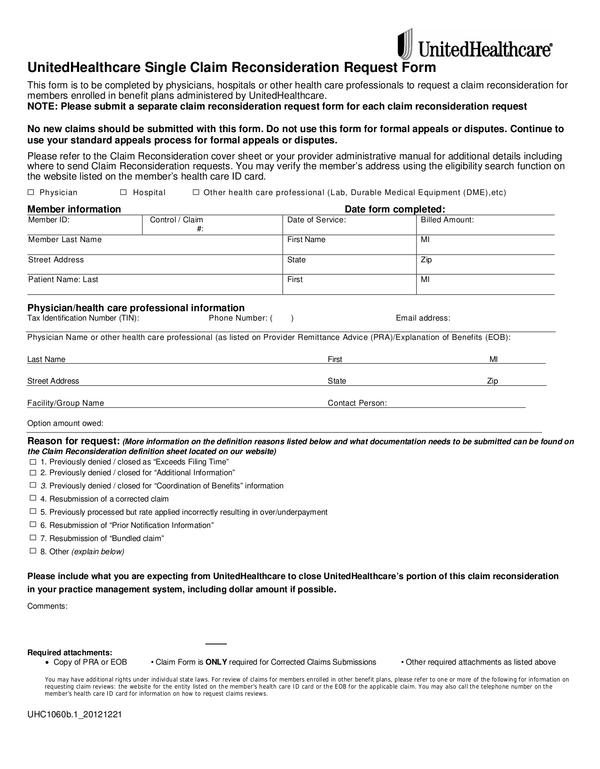
Once completed you can sign your fillable form or send for signing. Our claims process, mail or fax appeal forms to: Web © 2022 united healthcare services, inc. Single claim reconsideration/corrected claim request form this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. Easily sign the united healthcare provider appeal form 2022 with your finger. Use fill to complete blank online others pdf forms for free. All forms are printable and downloadable. Web this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact information and resources. • please submit a separate form for each claim
Web step 1 is to file a claim reconsideration request. Open the united healthcare reconsideration form and follow the instructions. Single claim reconsideration/corrected claim request form this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. Web an appeal is a request for a formal review of an adverse benefit decision. An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or that reduces of fails to make payment for benefits. Once completed you can sign your fillable form or send for signing. Use fill to complete blank online others pdf forms for free. Continue to use your standard process Web care provider administrative guides and manuals. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact information and resources.
Top United Healthcare Appeal Form Templates Free To Download In PDF
An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or that reduces of fails to make payment for benefits. Open the united healthcare reconsideration form and follow the instructions. Web step 1 is to file a claim reconsideration request. Step 2 is to file an appeal if you disagree with the outcome.

ads/responsive.txt Uhc Reconsideration form 2018 Best Of Luxury Card
The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact information and resources. An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or that reduces of fails to make payment for benefits. Web the unitedhealthcare provider portal allows you to submit referrals, prior authorizations, claims, claim.
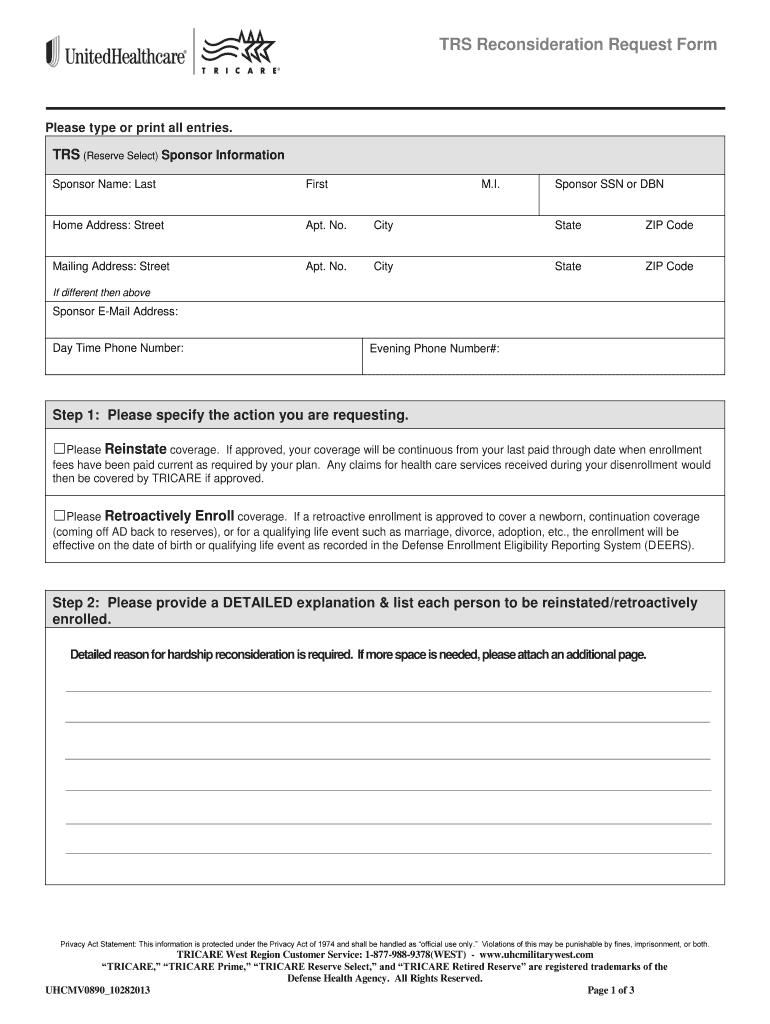
Triwest Reconsideration Form Fill Online, Printable, Fillable, Blank
All forms are printable and downloadable. Web © 2022 united healthcare services, inc. Web an appeal is a request for a formal review of an adverse benefit decision. Our claims process, mail or fax appeal forms to: An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or that reduces of fails to.

ads/responsive.txt Uhc Reconsideration form 2018 Lovely Humana Prior
You have 1 year from the date of occurrence to file an appeal with the nhp. Web care provider administrative guides and manuals. Single claim reconsideration/corrected claim request form this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. Web © 2022 united healthcare services, inc. • please submit.

ads/responsive.txt Uhc Reconsideration form 2018 Brilliant How to Write
Easily sign the united healthcare provider appeal form 2022 with your finger. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact information and resources. Web step 1 is to file a claim reconsideration request. Single claim reconsideration/corrected claim request form this form is to be completed by physicians, hospitals or other health care.
United Health Care Online at
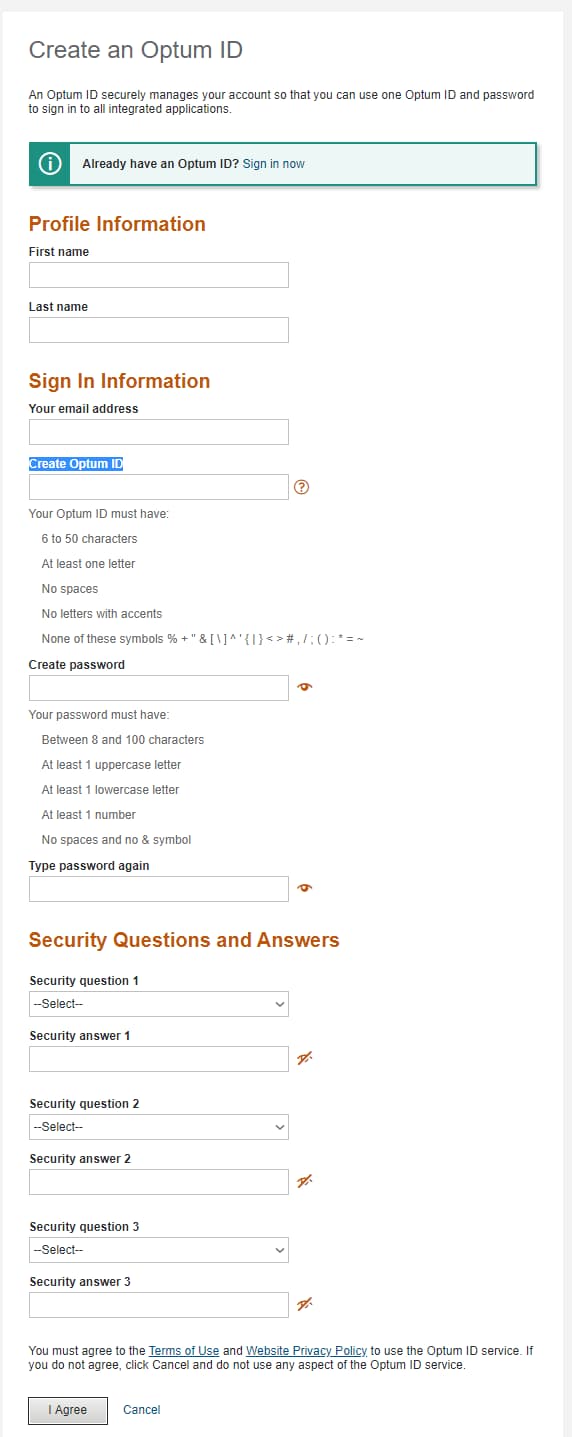
Open the united healthcare reconsideration form and follow the instructions. Web the unitedhealthcare provider portal allows you to submit referrals, prior authorizations, claims, claim reconsideration and appeals, demographic changes and more. Web step 1 is to file a claim reconsideration request. You have 1 year from the date of occurrence to file an appeal with the nhp. Our claims process,.

United Care Form Fill Online, Printable, Fillable, Blank pdfFiller
Web the unitedhealthcare provider portal allows you to submit referrals, prior authorizations, claims, claim reconsideration and appeals, demographic changes and more. Continue to use your standard process Web fill online, printable, fillable, blank uhc claim reconsideration request form. Use fill to complete blank online others pdf forms for free. Web step 1 is to file a claim reconsideration request.
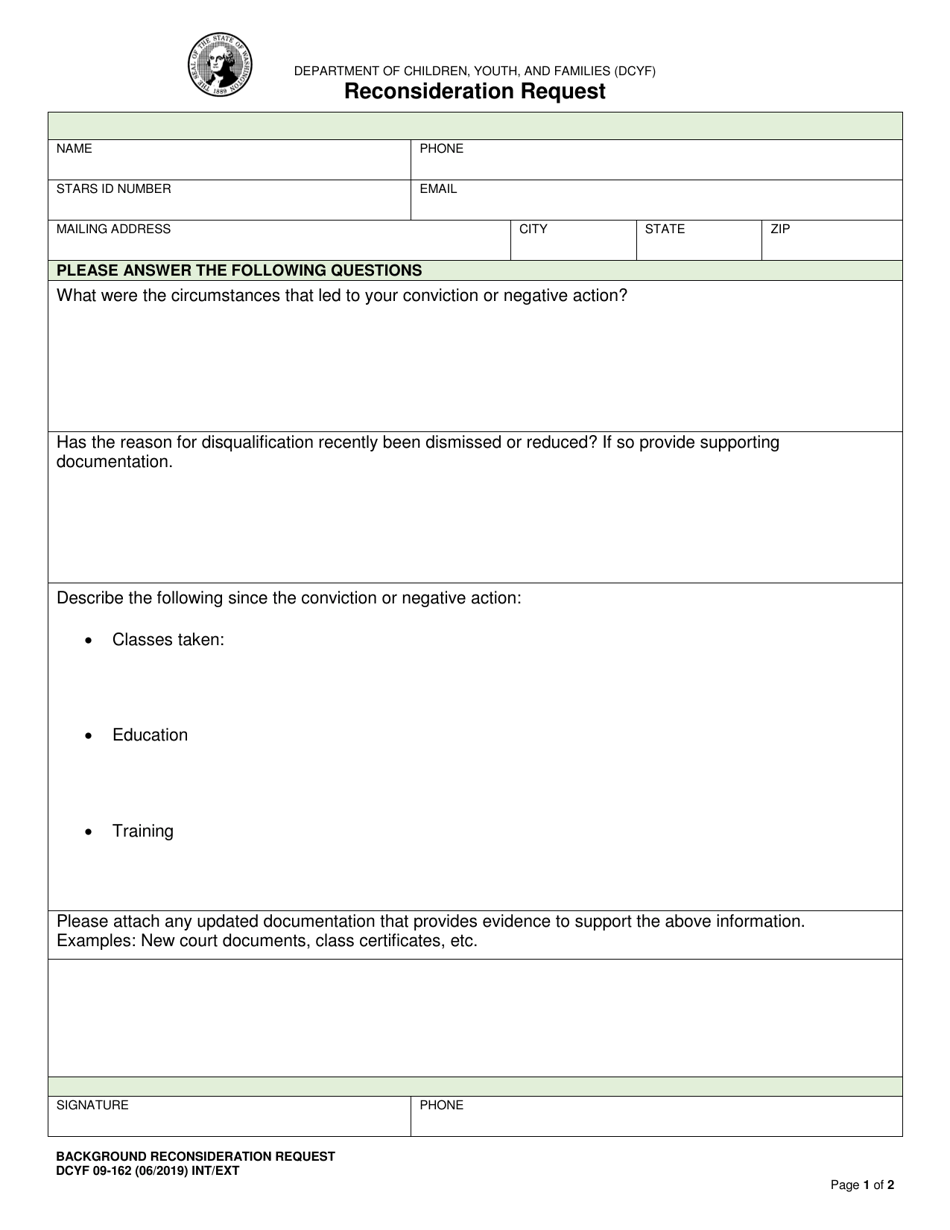
DCYF Form 09162 Download Fillable PDF or Fill Online Reconsideration
Step 2 is to file an appeal if you disagree with the outcome of the claim reconsideration decision. Open the united healthcare reconsideration form and follow the instructions. Web step 1 is to file a claim reconsideration request. Continue to use your standard process Web an appeal is a request for a formal review of an adverse benefit decision.

Uhc Reconsideration form 2018 Fresh Sample Proof Health Insurance
Web if you are unable to use the online reconsideration and appeals process outlined in chapter 10: Our claims process, mail or fax appeal forms to: Web © 2022 united healthcare services, inc. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact information and resources. All forms are printable and downloadable.

ads/responsive.txt Uhc Reconsideration form 2018 Elegant Favorite Claim
Web care provider administrative guides and manuals. Web an appeal is a request for a formal review of an adverse benefit decision. All forms are printable and downloadable. Easily sign the united healthcare provider appeal form 2022 with your finger. Web if you are unable to use the online reconsideration and appeals process outlined in chapter 10:
Send Filled & Signed United Healthcare Reconsideration Form 2022 Or Save.
Our claims process, mail or fax appeal forms to: Web this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. Web fill online, printable, fillable, blank uhc claim reconsideration request form. Web if you are unable to use the online reconsideration and appeals process outlined in chapter 10:
Web An Appeal Is A Request For A Formal Review Of An Adverse Benefit Decision.
You have 1 year from the date of occurrence to file an appeal with the nhp. Web step 1 is to file a claim reconsideration request. • please submit a separate form for each claim An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or that reduces of fails to make payment for benefits.
Once Completed You Can Sign Your Fillable Form Or Send For Signing.
Open the united healthcare reconsideration form and follow the instructions. Web © 2022 united healthcare services, inc. Web the unitedhealthcare provider portal allows you to submit referrals, prior authorizations, claims, claim reconsideration and appeals, demographic changes and more. Continue to use your standard process
The Following Links Provide Information Including, But Not Limited To, Prior Authorization, Processing Claims, Protocol, Contact Information And Resources.
Single claim reconsideration/corrected claim request form this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. • please submit a separate form for each claim • no new claims should be submitted with this form • do not use this form for formal appeals or disputes. Web care provider administrative guides and manuals. All forms are printable and downloadable.