Express Scripts Appeal Form
Express Scripts Appeal Form - Web include a copy of the claim decision, and. How to shield your express scripts claims form when doing it online? Web download pdf online application to submit a redetermination request form if you would like to request a coverage determination (such as an exception to the rules or restriction on our plan's coverage of a drug) or if you would like to make an appeal for us to reconsider a coverage decision, you may: You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination. Be postmarked or received by express scripts within a deadline of 90 calendar days from the date of the decision to: If you request an exception, your doctor must provide a statement to support your request. Web individual request electronic phi third party request for electronic protected health information to make a bulk request for electronic data, please download this form. Select the get form button on this page. Web drug, you have the right to ask us for a redetermination (appeal) of our decision. Web all you need to do is to pick the express scripts prior authorization, fill out the appropriate document parts, drag and drop fillable fields (if necessary), and certify it without having second guessing about whether or not your signed document is legally binding.
An express scripts prior authorization form is meant to be used by medical offices when requesting coverage for a patient’s prescription. The medical staff will need to fill out the form with the patient’s personal and medical details, as well the prescriber’s. Web download pdf online application to submit a redetermination request form if you would like to request a coverage determination (such as an exception to the rules or restriction on our plan's coverage of a drug) or if you would like to make an appeal for us to reconsider a coverage decision, you may: How to shield your express scripts claims form when doing it online? Web to initiate a coverage review request, please complete the form below and click submit. Web since your request for coverage of (or payment for) a prescription drug was denied, you have the right to ask us for a redetermination (appeal) of our decision. You will enter into our pdf editor. Representation documentation for requests made by someone other than the enrollee or the enrollee's prescriber: Web individual request electronic phi third party request for electronic protected health information to make a bulk request for electronic data, please download this form. This form may be sent to us by mail or fax:
If you request an exception, your doctor must provide a statement to support your request. This form may be sent to us by mail or fax: Web all you need to do is to pick the express scripts prior authorization, fill out the appropriate document parts, drag and drop fillable fields (if necessary), and certify it without having second guessing about whether or not your signed document is legally binding. Web express scripts prior (rx) authorization form. Web follow these steps to get your express scripts appeal edited for the perfect workflow: You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination. Web since your request for coverage of (or payment for) a prescription drug was denied, you have the right to ask us for a redetermination (appeal) of our decision. Web download pdf online application to submit a redetermination request form if you would like to request a coverage determination (such as an exception to the rules or restriction on our plan's coverage of a drug) or if you would like to make an appeal for us to reconsider a coverage decision, you may: How to shield your express scripts claims form when doing it online? You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination.

Express Scripts Appeal Form Fill Online, Printable, Fillable, Blank
You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination. Web follow these steps to get your express scripts appeal edited for the perfect workflow: Select the get form button on this page. Representation documentation for requests made by someone other than the enrollee or the enrollee's.

Express Scripts Headquarters and Technology & Innovation Center
Be postmarked or received by express scripts within a deadline of 90 calendar days from the date of the decision to: Web individual request electronic phi third party request for electronic protected health information to make a bulk request for electronic data, please download this form. You have 60 days from the date of our notice of denial of medicare.

Free Express Scripts Prior (Rx) Authorization Form PDF eForms
You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination. How to shield your express scripts claims form when doing it online? The medical staff will need to fill out the form with the patient’s personal and medical details, as well the prescriber’s. Web express scripts prior.

57 HQ Images Express Scripts Appeal Form Express Scripts Prior
Representation documentation for requests made by someone other than the enrollee or the enrollee's prescriber: You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination. Web individual request electronic phi third party request for electronic protected health information to make a bulk request for electronic data, please.
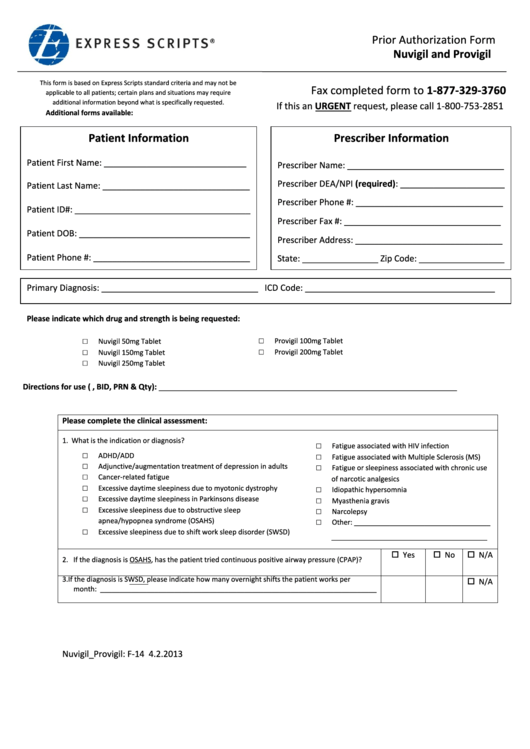
Express Scripts Prior Authorization Form Nuvigil And Provigil
This form may be sent to us by mail or fax: Web download pdf online application to submit a redetermination request form if you would like to request a coverage determination (such as an exception to the rules or restriction on our plan's coverage of a drug) or if you would like to make an appeal for us to reconsider.
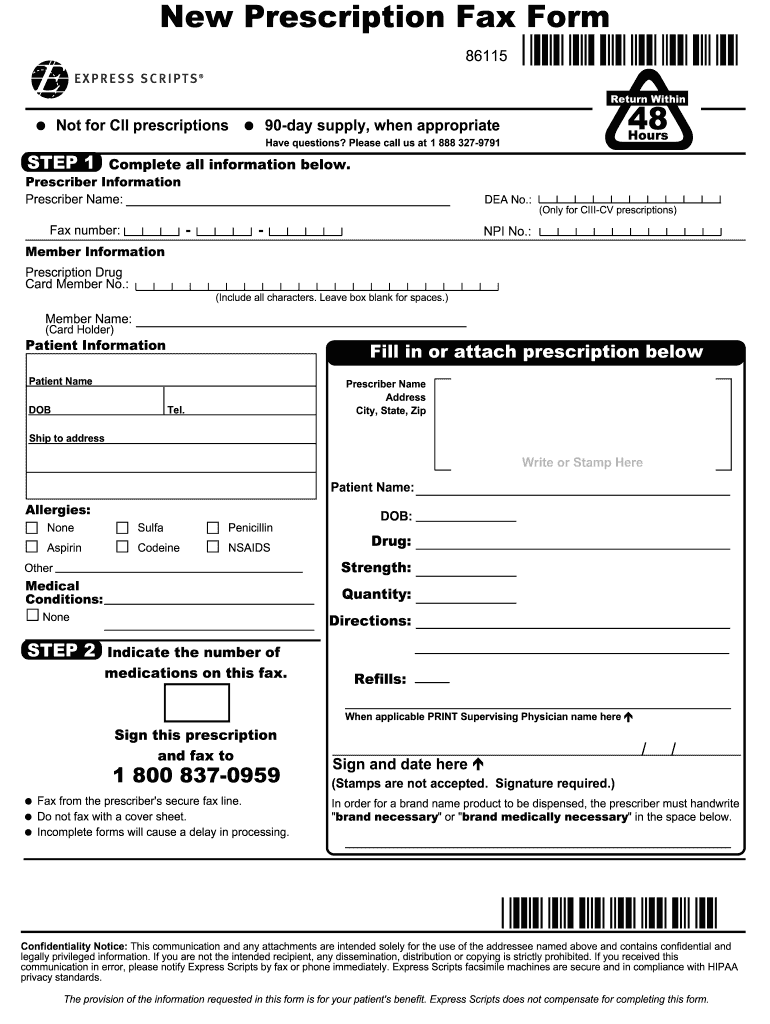
Express Scripts New Prescription Fax Form Fill and Sign Printable
You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination. Enrollee/requestor information complete this section only if the person making this request is not the enrollee or prescriber: If you request an exception, your doctor must provide a statement to support your request. An express scripts prior.

57 HQ Images Express Scripts Appeal Form Express Scripts Prior
Web download pdf online application to submit a redetermination request form if you would like to request a coverage determination (such as an exception to the rules or restriction on our plan's coverage of a drug) or if you would like to make an appeal for us to reconsider a coverage decision, you may: If you request an exception, your.
Express Scripts Fax Forms for Physicians Prior Authorization Fill Out
The medical staff will need to fill out the form with the patient’s personal and medical details, as well the prescriber’s. You will enter into our pdf editor. Web since your request for coverage of (or payment for) a prescription drug was denied, you have the right to ask us for a redetermination (appeal) of our decision. Web to initiate.
How to Get Prescription Refill Home
This form may be sent to us by mail or fax: Enrollee/requestor information complete this section only if the person making this request is not the enrollee or prescriber: You may submit more documentation to support your appeal. Representation documentation for requests made by someone other than the enrollee or the enrollee's prescriber: Web express scripts prior (rx) authorization form.
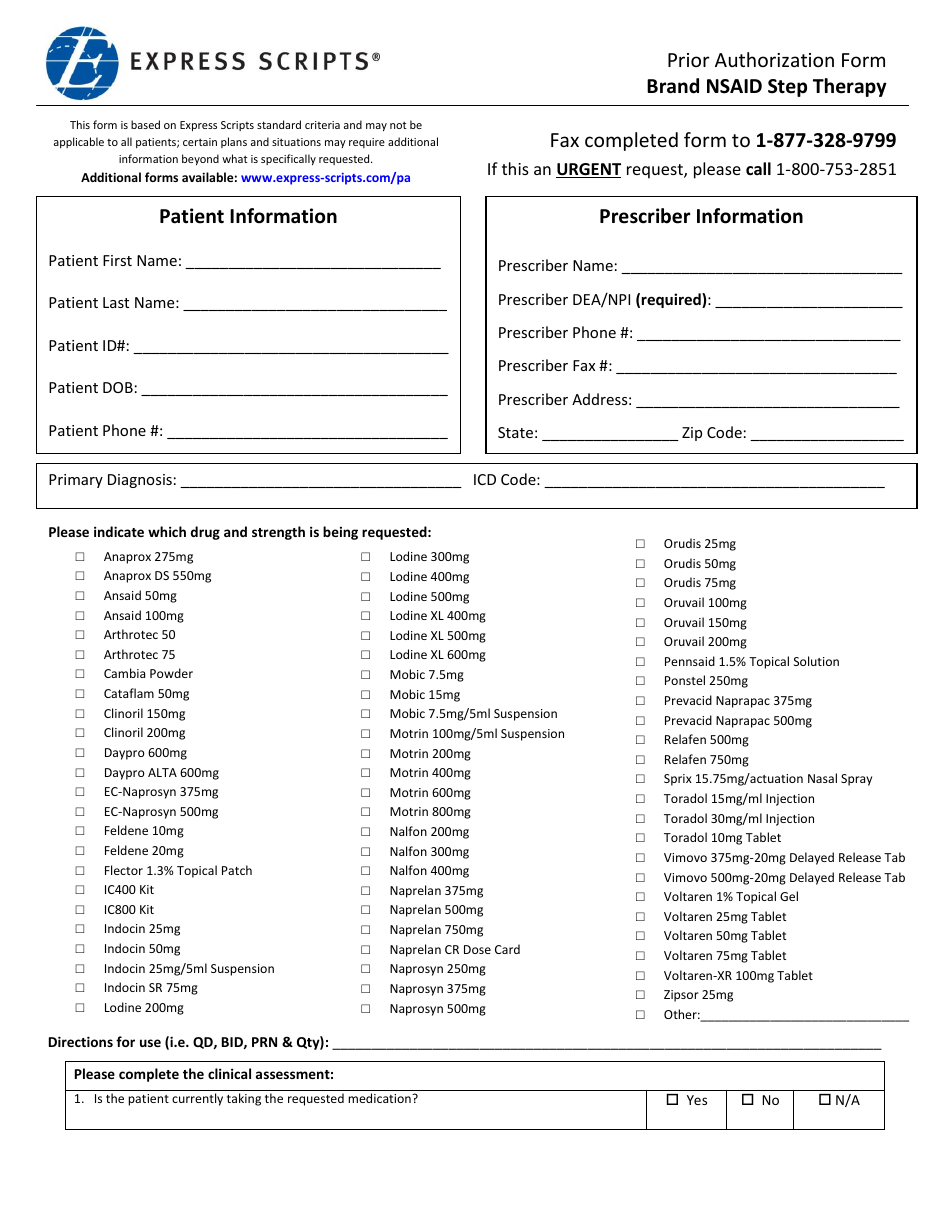
Prior Authorization Form Brand Nsaid Step Therapy Express Scripts
You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination. Enrollee/requestor information complete this section only if the person making this request is not the enrollee or prescriber: You may submit more documentation to support your appeal. You will enter into our pdf editor. How to shield.
You Will Enter Into Our Pdf Editor.
Be postmarked or received by express scripts within a deadline of 90 calendar days from the date of the decision to: If you request an exception, your doctor must provide a statement to support your request. The medical staff will need to fill out the form with the patient’s personal and medical details, as well the prescriber’s. Web all you need to do is to pick the express scripts prior authorization, fill out the appropriate document parts, drag and drop fillable fields (if necessary), and certify it without having second guessing about whether or not your signed document is legally binding.
Web Download Pdf Online Application To Submit A Redetermination Request Form If You Would Like To Request A Coverage Determination (Such As An Exception To The Rules Or Restriction On Our Plan's Coverage Of A Drug) Or If You Would Like To Make An Appeal For Us To Reconsider A Coverage Decision, You May:
Web individual request electronic phi third party request for electronic protected health information to make a bulk request for electronic data, please download this form. Representation documentation for requests made by someone other than the enrollee or the enrollee's prescriber: This form may be sent to us by mail or fax: Enrollee/requestor information complete this section only if the person making this request is not the enrollee or prescriber:
You Have 60 Days From The Date Of Our Notice Of Denial Of Medicare Prescription Drug Coverage To Ask Us For A Redetermination.
An express scripts prior authorization form is meant to be used by medical offices when requesting coverage for a patient’s prescription. Web include a copy of the claim decision, and. Web drug, you have the right to ask us for a redetermination (appeal) of our decision. Web since your request for coverage of (or payment for) a prescription drug was denied, you have the right to ask us for a redetermination (appeal) of our decision.
How To Shield Your Express Scripts Claims Form When Doing It Online?
Select the get form button on this page. Web express scripts prior (rx) authorization form. You may submit more documentation to support your appeal. You have 60 days from the date of our notice of denial of medicare prescription drug coverage to ask us for a redetermination.