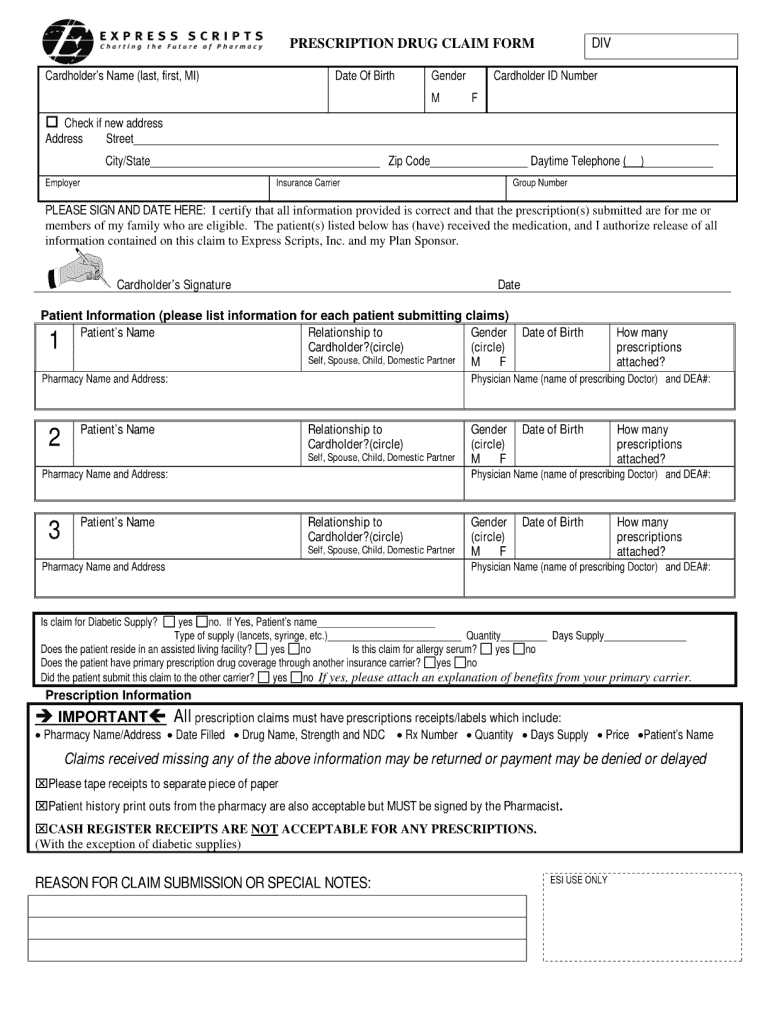
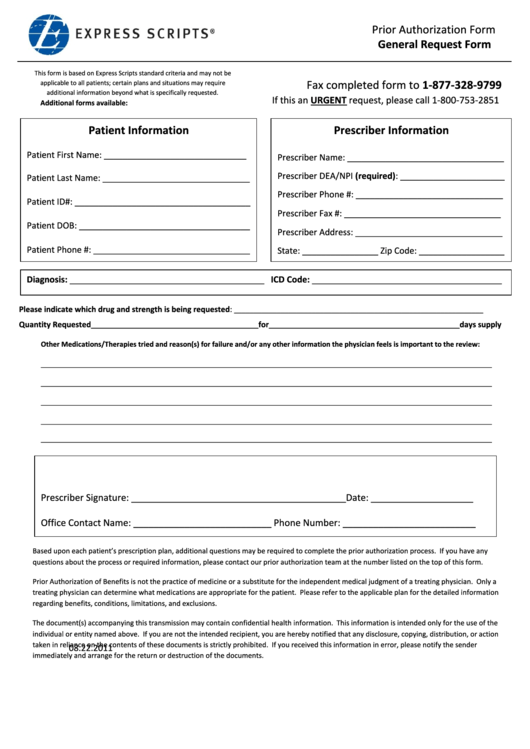
Express Scripts General Request Form
Express Scripts General Request Form - Please indicate which drug and strength is being requested: If you want another individual (such as a family member or friend) to make a request for you, that individual must be your representative. Your prescriber may ask us for a coverage determination on your behalf. Save or instantly send your ready documents. Contact us to learn how to name a representative. Call us at 800.753.2851, download a state specific fax form or fax your requests to the number shown on our general request form. 24 hours a day, 7 days a week. Web communication in error, please notify express scripts by fax or phone immediately. Prior authorization form for physicians in arkansas, michigan, oregon, and vermont. Medicare plan members coverage review information
If you can't submit a request via telephone, please use our general request form or one of the state specific forms below and fax it to the number on the form. Your prescriber may ask us for a coverage determination on your behalf. Web communication in error, please notify express scripts by fax or phone immediately. Web prior authorization criteria is available upon request. We have pharmacists or service representatives available 24/7 to help answer your health and insurance questions. Call us at 800.753.2851, download a state specific fax form or fax your requests to the number shown on our general request form. Who may make a request: Web complete express scripts general request form online with us legal forms. Express scripts does not compensate for completing this form. The provision of the information requested in this form is for your patient's benefit.
Web call for help with your prescription benefit or prescriptions filled through the express scripts ® pharmacy. 24 hours a day, 7 days a week. Express scripts facsimile machines are secure and in compliance with hipaa privacy standards. Web we are here for you 24/7. Save or instantly send your ready documents. Web if you’re unable to use epa, there are other ways to submit your pa request. Please indicate which drug and strength is being requested: If you want another individual (such as a family member or friend) to make a request for you, that individual must be your representative. Web communication in error, please notify express scripts by fax or phone immediately. Your prescriber may ask us for a coverage determination on your behalf.
Express Scripts Fax Forms for Physicians Prior Authorization Fill Out
Web communication in error, please notify express scripts by fax or phone immediately. Contact us to learn how to name a representative. 24 hours a day, 7 days a week. Web complete express scripts general request form online with us legal forms. Web prior authorization criteria is available upon request.

Express Scripts for Android APK Download
Call us at 800.753.2851, download a state specific fax form or fax your requests to the number shown on our general request form. We have pharmacists or service representatives available 24/7 to help answer your health and insurance questions. Who may make a request: The provision of the information requested in this form is for your patient's benefit. Please indicate.
Express Scripts And Prior Authorization Form Fill Out and Sign
Your prescriber may ask us for a coverage determination on your behalf. Call us at 800.753.2851, download a state specific fax form or fax your requests to the number shown on our general request form. Prior authorization form for physicians in arkansas, michigan, oregon, and vermont. 24 hours a day, 7 days a week. Web if you’re unable to use.

Express Scripts Appeal Form Fill Online, Printable, Fillable, Blank
Web individual request for electronic protected health information to access your electronic data, please download this form. An express scripts prior authorization form is meant to be used by medical offices when requesting coverage for a patient’s prescription. Web prior authorization criteria is available upon request. Contact us to learn how to name a representative. Please indicate which drug and.
Express Scripts Prior Authorization Form General Request Form
Please indicate which drug and strength is being requested: Web complete express scripts general request form online with us legal forms. Express scripts does not compensate for completing this form. If you want another individual (such as a family member or friend) to make a request for you, that individual must be your representative. Web express scripts prior (rx) authorization.
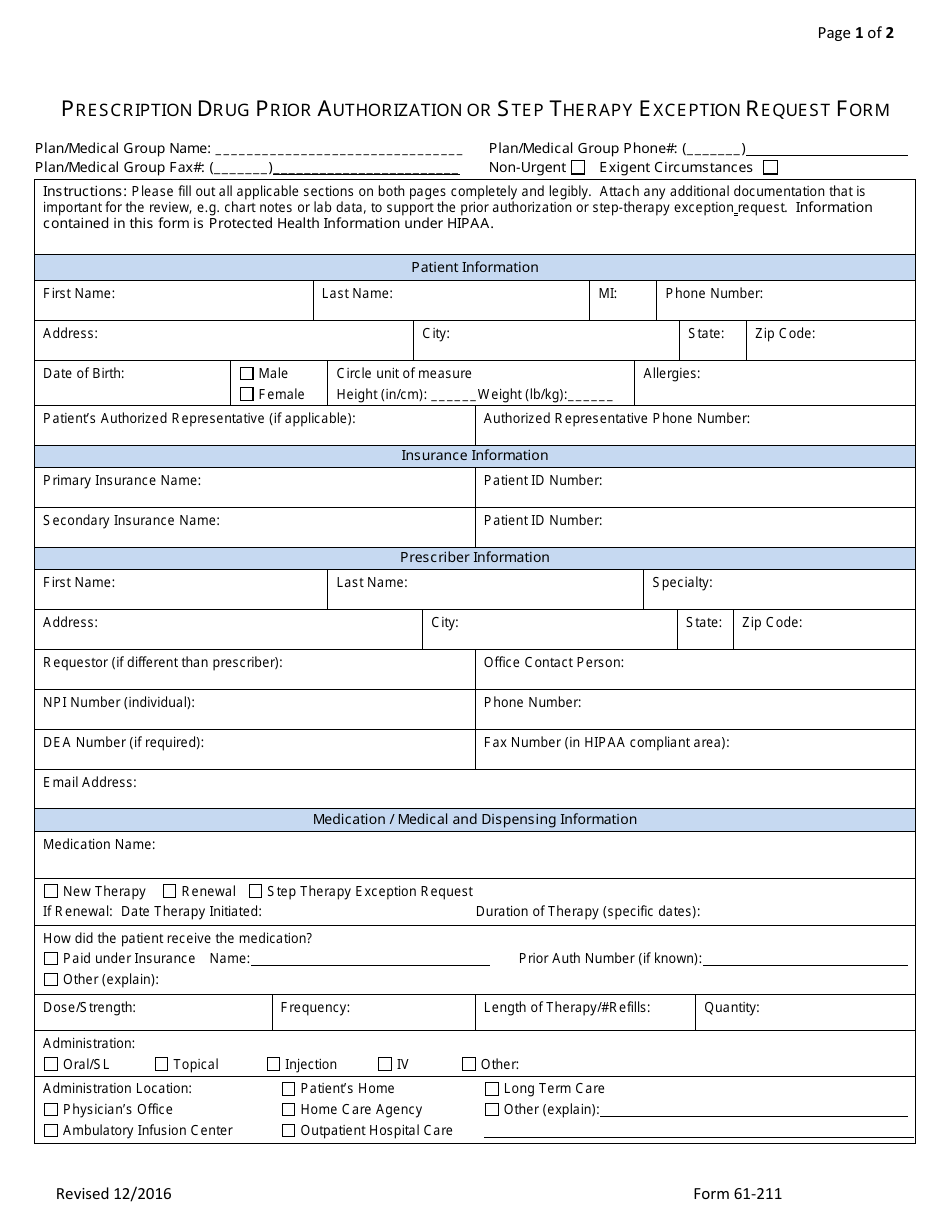
Form 61211 Download Fillable PDF or Fill Online Prescription Drug
Visit this page for state specific forms and pa statistics download general request form; Express scripts facsimile machines are secure and in compliance with hipaa privacy standards. We have pharmacists or service representatives available 24/7 to help answer your health and insurance questions. Please indicate which drug and strength is being requested: Your prescriber may ask us for a coverage.
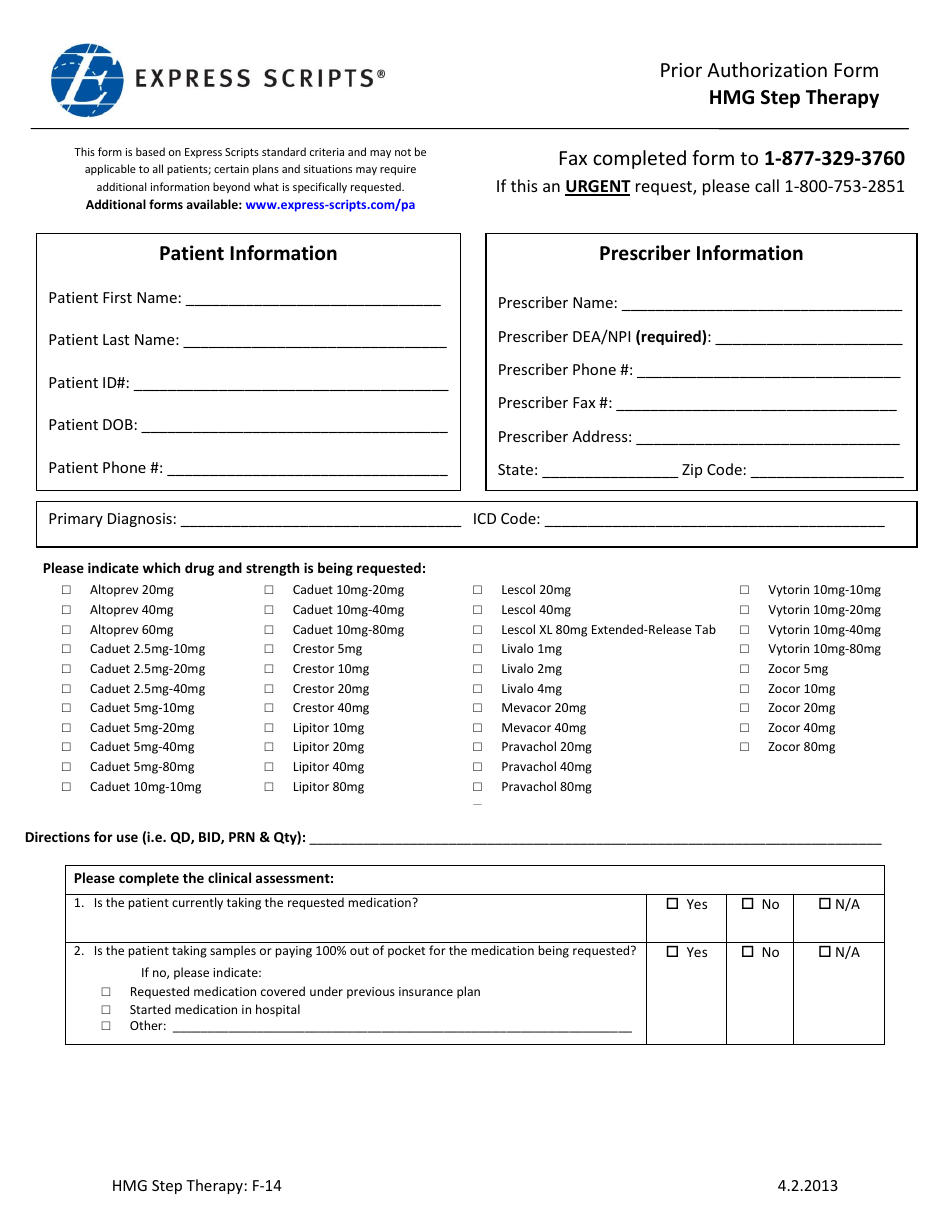
Form F14 Download Printable PDF or Fill Online Prior Authorization Form
We have pharmacists or service representatives available 24/7 to help answer your health and insurance questions. Easily fill out pdf blank, edit, and sign them. Express scripts facsimile machines are secure and in compliance with hipaa privacy standards. If you can't submit a request via telephone, please use our general request form or one of the state specific forms below.

Express Scripts forms Elegant This
Express scripts facsimile machines are secure and in compliance with hipaa privacy standards. Web individual request for electronic protected health information to access your electronic data, please download this form. We have pharmacists or service representatives available 24/7 to help answer your health and insurance questions. 24 hours a day, 7 days a week. Web communication in error, please notify.
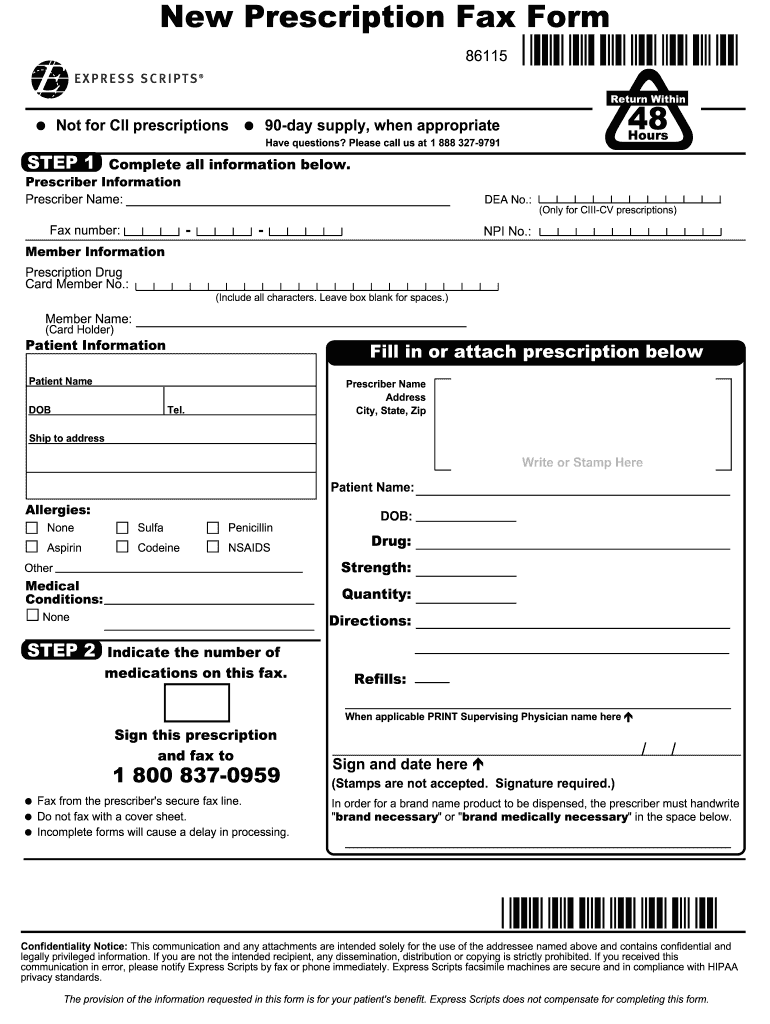
Express Scripts New Prescription Fax Form Fill and Sign Printable
The provision of the information requested in this form is for your patient's benefit. Web communication in error, please notify express scripts by fax or phone immediately. Medicare plan members coverage review information Web complete express scripts general request form online with us legal forms. If you can't submit a request via telephone, please use our general request form or.
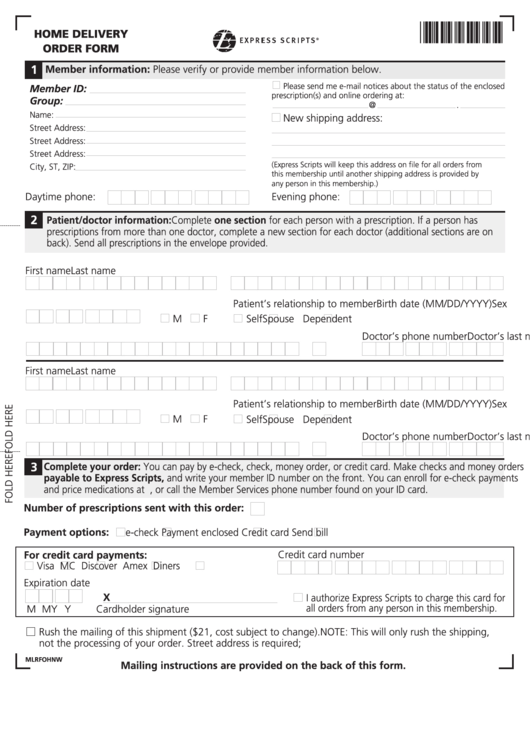
Express Scripts MailOrder Form printable pdf download
Web we are here for you 24/7. Call us at 800.753.2851, download a state specific fax form or fax your requests to the number shown on our general request form. Your prescriber may ask us for a coverage determination on your behalf. Web communication in error, please notify express scripts by fax or phone immediately. Web if you’re unable to.
Web We Are Here For You 24/7.
Visit this page for state specific forms and pa statistics download general request form; Who may make a request: Web express scripts prior (rx) authorization form. An express scripts prior authorization form is meant to be used by medical offices when requesting coverage for a patient’s prescription.
Your Prescriber May Ask Us For A Coverage Determination On Your Behalf.
Web if you’re unable to use epa, there are other ways to submit your pa request. Web prior authorization criteria is available upon request. Save or instantly send your ready documents. Express scripts does not compensate for completing this form.
Call Us At 800.753.2851, Download A State Specific Fax Form Or Fax Your Requests To The Number Shown On Our General Request Form.
Please indicate which drug and strength is being requested: Web call for help with your prescription benefit or prescriptions filled through the express scripts ® pharmacy. Express scripts facsimile machines are secure and in compliance with hipaa privacy standards. The provision of the information requested in this form is for your patient's benefit.
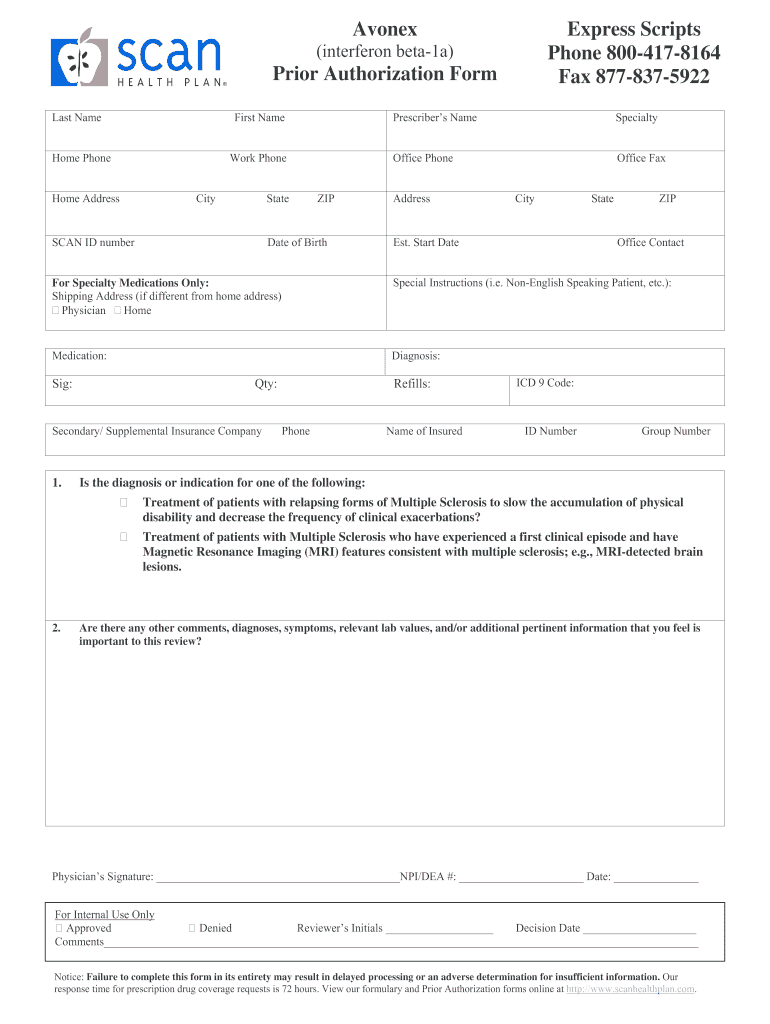
Prior Authorization Form For Physicians In Arkansas, Michigan, Oregon, And Vermont.
Web complete express scripts general request form online with us legal forms. Contact us to learn how to name a representative. We have pharmacists or service representatives available 24/7 to help answer your health and insurance questions. Medicare plan members coverage review information